Download
1 / 1
10 likes | 136 Vues
Racial and Ethnic Differences in Nationwide Utilization of Cardiac Resynchronization Therapy.

E N D
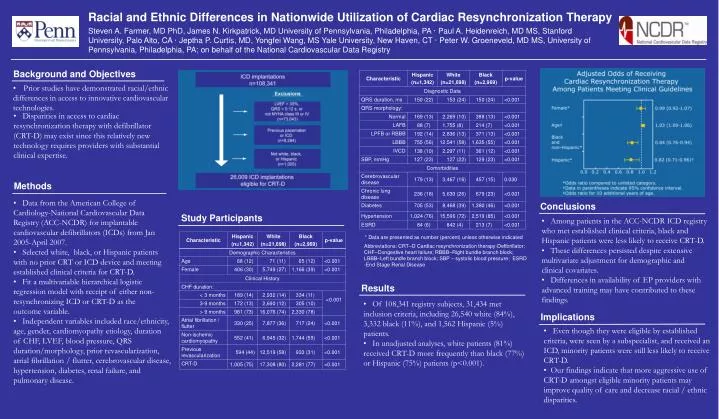
Racial and Ethnic Differences in Nationwide Utilization of Cardiac Resynchronization Therapy Steven A. Farmer, MD PhD, James N. Kirkpatrick, MD University of Pennsylvania, Philadelphia, PA · Paul A. Heidenreich, MD MS, Stanford University, Palo Alto, CA · Jeptha P. Curtis, MD, Yongfei Wang, MS Yale University, New Haven, CT · Peter W. Groeneveld, MD MS, University of Pennsylvania, Philadelphia, PA; on behalf of the National Cardiovascular Data Registry Background and Objectives • Prior studies have demonstrated racial/ethnic differences in access to innovative cardiovascular technologies. • Disparities in access to cardiac resynchronization therapy with defibrillator (CRT-D) may exist since this relatively new technology requires providers with substantial clinical expertise. Methods • Data from the American College of Cardiology-National Cardiovascular Data Registry (ACC-NCDR) for implantable cardiovascular defibrillators (ICDs) from Jan 2005-April 2007. • Selected white, black, or Hispanic patients with no prior CRT or ICD device and meeting established clinical criteria for CRT-D. • Fit a multivariable hierarchical logistic regression model with receipt of either non-resynchronizing ICD or CRT-D as the outcome variable. • Independent variables included race/ethnicity, age, gender, cardiomyopathy etiology, duration of CHF, LVEF, blood pressure, QRS duration/morphology, prior revascularization, atrial fibrillation / flutter, cerebrovascular disease, hypertension, diabetes, renal failure, and pulmonary disease. Conclusions Study Participants • Among patients in the ACC-NCDR ICD registry who met established clinical criteria, black and Hispanic patients were less likely to receive CRT-D. • These differences persisted despite extensive multivariate adjustment for demographic and clinical covariates. • Differences in availability of EP providers with advanced training may have contributed to these findings. * Data are presented as number (percent) unless otherwise indicated. Abbreviations: CRT–D Cardiac resynchronization therapy-Defibrillator; CHF–Congestive heart failure; RBBB–Right bundle branch block; LBBB–Left bundle branch block; SBP – systolic blood pressure; ESRD -End Stage Renal Disease Results • Of 108,341 registry subjects, 31,434 met inclusion criteria, including 26,540 white (84%), 3,332 black (11%), and 1,562 Hispanic (5%) patients. • In unadjusted analyses, white patients (81%) received CRT-D more frequently than black (77%) or Hispanic (75%) patients (p<0.001). Implications • Even though they were eligible by established criteria, were seen by a subspecialist, and received an ICD, minority patients were still less likely to receive CRT-D. • Our findings indicate that more aggressive use of CRT-D amongst eligible minority patients may improve quality of care and decrease racial / ethnic disparities.