Download
1 / 43
460 likes | 544 Vues
Anterior Glenohumeral Instability. Christian Veillette M.D., M.Sc., FRCSC Assistant Professor, University of Toronto Shoulder & Elbow Reconstructive Surgery Toronto Western Hospital University Health Network Email: orthonet@gmail.com. Objectives. Epidemiology Natural History Pathoanatomy

E N D
Anterior Glenohumeral Instability Christian Veillette M.D., M.Sc., FRCSC Assistant Professor, University of Toronto Shoulder & Elbow Reconstructive Surgery Toronto Western Hospital University Health Network Email: orthonet@gmail.com
Objectives • Epidemiology • Natural History • Pathoanatomy • Diagnosis • History, Physical Exam, Imaging • Management Options • Consideration, Indications, Complications • Surgical Procedures • Cases
Introduction • Incidence – 2% over lifetime - Hovelius (CORR 1982); Simonet (CORR 1984) • Anterior dislocations account for ~95% of shoulder dislocations • Typically occurs in athletes who are < 25 years old • Males are much more commonly affected than are females (85-90%) • Pathology most commonly found in shoulders following a dislocation is a Bankart lesion • Disruption of the labrum and the contiguous anterior band of the inferior glenohumeral ligamentous complex (IGHLC) • Bankhart lesion occurs > 85% of the time
Mechanism of Injury • Most common mechanism of injury is a fall onto an outstretched arm • Extremity is typically in an externally rotated and abducted position • Places the anterior structures at greatest risk for failure (especially the inferior glenohumeral ligament) • Other mechanisms: • elevation combined with external rotation • direct blow
Classification • Instability can be classified by: • direction of instability (anterior, posterior, multidirectional) • degree of instability (subluxation, dislocation) • etiology (traumatic, atraumatic, overuse) • timing (acute, recurrent, fixed) • TUBS and AMBRI (Matsen) • TUBS or “Torn Loose” • Traumatic aetiology, Unidirectional instability, Bankart lesion is the pathology, Surgery is required • AMBRI or “Born Loose” • Atraumatic: minor trauma, Multidirectional instability may be present, Bilateral: asymptomatic shoulder is also loose, Rehabilitation is the treatment of choice, Inferior capsular shift: surgery required if conservative measures fail
Prognostic variables • Gender – No correlation if look at <30 yrs of age group • Hand dominance - No correlation consistently reported • Initial Trauma - Controversial whether amount of initial trauma correlates with recurrence • Sports participation - Likely that level and type of sport participation correlates with recurrence rate • Initial X-ray Appearance – GT # low rate • Period of immobilsation – Unclear whether period of immobilization corrrelates with recurrence rate • Age – Strong correlation between age and recurrence in all studies
Age & Recurrence Rate • McLaughlin and Cavallaro (Am J Surg 1950) • 573 patients - 90% in patients < 20 y, 60% in patients 20-40 y, only 10% in patients > 40 y • Rowe (Orthop Clin North Am 1980) • 94% in patients < 20 y, 74% in patients 20-40 y • Henry and Genung (Am J Sports Med 1982) • 121 patients - 88% regardless of type of nonoperative treatment • Simonet and Cofield (Am J Sports Med 1984) • 116 patients - 66% in patients < 20 y, 40% in patients 20-40 y • Arciero et al (Am J Sports Med 1984) • 80% in 15 student-athletes with average age of 20 y
Natural History • Bilaterality - <30 y at time of first dislocation • 18% bilaterality within 10 yrs (Hovelius, JBJS 1996) • Osteoarthritis - Risk of OA regardless of recurrence or surgery at 10 y • mod. to severe 9% (Hovelius, JBJS 1996) • mild 11% • 17% (Lill, Chirurg 1998) • Functional Disability (Tsai et al, Am J Sports Med 1991) • ~ 60% of patients with anterior instability complained of poor strength, decrease range of motion, increased pain after conservative treatment
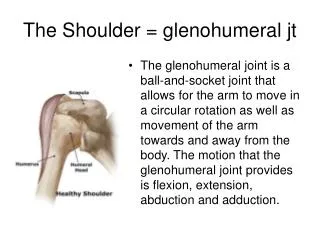
Anatomy • humeral head is retroverted 30o • typical neck-shaft angle is 130o • glenoid fossa average radius of curvature is 24 mm, only 2 mm less than humeral head • less than one-third of the humeral head articulates with glenoid during any given position of rotation • glenohumeral articulation is minimally constrained by bony anatomy alone • glenoid labrum is a fibrocartilaginous structure • functionally deepens the glenoid fossa • serves as an anatomic restraint to humeral head translation • provides an anchor point for the glenohumeral ligaments • stability is conferred by a series of dynamic and static soft tissue restraints
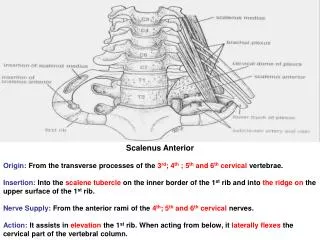
Shoulder Stabilisers - Static • Intracapsular pressure • Suction effect: glenoid labrum acting on humeral head like a “plunger” • Adhesion-cohesion: between 2 wet smooth surfaces • Glenoid version • Humeral retroversion: normal 21-30º, some studies have shown a significant reduction in patients with recurrent anterior dislocation • Labrum: “chock block” to humeral head movement, increases depth of the glenoid by 50% • Ligaments – main static restraints • Coracohumeral ligament • Superior glenohumeral ligament (SGHL) • Middle glenohumeral ligament (MGHL) • Inferior glenohumeral ligament complex (IGHLC) – “hammock” • Posterosuperior capsule Primary static stabilizer limiting anterior movement of the shoulder in 90 degrees of abduction is the IGHL complex
Shoulder Stabilisers - Dynamic • Rotator cuff • Subscapularis muscle provides stability at lower degrees of abduction but contributes little when shoulder is in 90o abduction • Rotator cuff compresses humeral head into glenolabral socket, contributing stability, esp. in middle ROM when ligaments are lax • Proprioception • Lephart et al 1994 studied proprioception in three groups of patients: Normal, Unstable, Reconstructed shoulders • Proprioception was significantly reduced in unstable shoulders but returned to near normal in reconstructed shoulders • Long head of biceps: biceps is much more active in patients with recurrent dislocation
Pathophysiology • pathologic lesions leading to the unstable shoulder can be divided into two main groups: • anterior labrum • glenohumeral capsule
Anterior Labrum • Bankart lesion • classically described as the detachment of the anteroinferior labrum with its attached inferior glenohumeral ligament complex • Initially felt that this detachment was the “essential lesion” • Speer et al. • Created Bankhart lesion from 12 o’clock to 6 o’clock and found minimal translation (<4 mm) • Capsular injury also required to dislocate shoulder
Glenohumeral Capsule • Turkel 1981 • Selective cutting study showed importance of GH ligaments • Bigliani et al. 1992 • Cadaveric bone-ligament-bone specimens of the IGHL were created and tested to failure • found that ligament failed • off the glenoid in 40% of the specimens (Bankart) • intrasubstance in 35% • off the humeral side in 25% • Most importantly showed that the capsule underwent plastic deformation prior to failure in all specimens
Patient History • Mechanism of injury is critical in management of dislocated shoulder • Arm position at time of injury helpful in subtle forms of subluxation • if the patient complains of symptoms in the cocking position, anterior subluxation • if the symptoms occur in the follow-through phase, posterior subluxation • Identify the amount of force required • Number of dislocations suffered by the patient • Age at the time of first dislocation is extremely important • most important prognostic indicator for patients with recurrent dislocations.
Exam - Acute Instability • Patients present with severe pain with arm held at side • Normal contour of deltoid and acromion are usually lost • Visual inspection, palpation, strength testing and a thorough neurovascular examination • Specific neurologic testing should include pre-reduction evaluation of axillary, musculocutaneous, median, ulnar, and radial nerves. • Sensation over axillary nerve distribution (lateral aspect of the shoulder) has proven to be quite unreliable. • Isometric contraction of 3 deltoid heads (anterior, middle, and posterior), usually indicates an intact axillary nerve.
Exam - Recurrent Instability • Apprehension test • Anterior release • Anteroposterior translation • Grade 1+ translation to the glenoid rim • Grade 2+ the head subluxes beyond the rim but self-reduces when the force is released • Grade 3+ the head dislocates and does not spontaneously reduce • Sulcus • Ligamentous laxity
Imaging Acute Setting • a true anteroposterior (AP) view, trans-scapular Y view, and axillary view should be obtained to determine the direction of the dislocation • Radiographs should be performed before reduction is attempted unless • the direction of dislocation is known from prior dislocations • the reduction is performed by an experienced physician, trainer, or other health care worker. • Post-reduction radiographs should confirm that the reduction was successful and that there are no acute fractures
Imaging Recurrent Instability • Several special views may be more helpful with recurrent instability • AP radiograph in internal rotation, Stryker-notch views are used to visualize Hill-Sachs lesion • West Point axillary view used to visualize anteroinferior glenoid (Bankart), avoids superimposition of the coracoid process & clavicle
Intra-articular lidocaine vs. IV sedation for closed reduction? Miller et. al. J Bone Joint Surg Am. 2002 Dec;84-A(12):2135-9. • prospective, randomized study, skeletally mature patients, isolated glenohumeral joint dislocation • IV sedation or intra-articular lidocaine, modified Stimson method • 30 patients • lidocaine group (n=15) - significantly less time in ER (av. time, 75 min vs 185 min in the sedation group, p < 0.01) • no significant difference between groups with regard to pain (p = 0.37), success of Stimson technique (p = 1.00), or time required to reduce shoulder (p = 0.42) • cost of IV sedation was $97.64/patient vs $0.52 for intra-articular lidocaine • Use of intra-articular lidocaine to facilitate reduction with the Stimson technique • safe and effective method • less money, time, and nursing resources
Orlinsky et. al. J Emerg Med. 2002 Apr;22(3):241-5. • compare the analgesic effectiveness of intra-articular lidocaine versus intravenous meperidine and diazepam • Prospective randomized trial • 54 patients with anterior shoulder dislocations • 29 intra-articular lidocaine (IAL) • 25 intravenous meperidine/diazepam (IVMD) • IAL less effective than IVMD in relieving pre-reduction pain (p = 0.045) • IAL equally effective in overall pain relief (p = 0.98) • IAL was more effective than IVMD in shortening recovery time (p = 0.025) • IVMD trend towards physician-perceived muscle relaxation and patient's perception of analgesia adequacy
Kosnik et. Al. Am J Emerg Med. 1999 Oct;17(6):566-70. • prospective, randomized, nonblinded clinical trial • local intraarticular lidocaine injection (IAL) vs intravenous analgesia/sedation (IVAS) • Level 1, trauma center • 49 patients: 20 - IVAS group, 29 - IAL group • No difference between pain scores (IVAS 3.32+/-2.39 vs IAL 4.90+/-2.34, P = .18) • No difference between ease of reduction scores (IVAS 3.32+/-2.36 vs IAL 4.45+/-2.46, P = .12) • IVAS tended to have higher success rate (20 of 20) than IAL (25 of 29) (P = .16). • Reduction rate as a function of time delay in treatment • patients presenting 5.5 h after dislocation more likely to fail treatment with IAL (P = .00001) • Half of the patients in the IAL group who had experience with IVAS did not favor IAL
Is Sling Appropriate? • Non-operative management = Sling immobilzation with the arm internally rotated No evidence • Itoi et al. J Bone Joint Surg Am 2001; 83-A(5): 661-667 • magnetic resonance imaging in patients • Hatrick C, O'Leary S, Miller B, et al. ORS 2002. • load sensors in cadavers
Itoi et. al. J Shoulder Elbow Surg. 2003 Sep-Oct;12(5):413-5. • Prospective, nonrandomized trial • 40 patients initial shoulder dislocations • Immobilization in internal rotation (IR group, n = 20) • Immobilization in external rotation (ER group, n = 20) • Recurrence rate @ 15.5 months • 30% in the IR group • 0% in the ER group • Difference in recurrence rate was even greater < 30 years • 45% in the IR group • 0% in the ER group
Role of Early Arthroscopic Repair? Bottoni et. al. Am J Sports Med. 2002 Jul-Aug;30(4):576-80. • Prospective, randomized clinical trial. Army Medical center. • Compared nonoperative treatment with arthroscopic Bankart repair for acute, traumatic shoulder dislocations in young athletes • 14 nonoperatively treated patients - 4 weeks of immobilization + supervised rehab. program • 10 operatively treated patients - arthroscopic Bankart repair (bioabsorbable tack) + same rehab protocol as nonop. patients • Av. follow-up = 36 months, 3 patients lost to follow-up • 9/12 nonoperatively treated patients (75%) developed recurrent instability • 6/9 required subsequent open Bankart repair for recurrent instability • 1/9 operatively treated patients (11.1%) developed recurrent instability
Kirkley A, Griffin S, Richards C, Miniaci A, Mohtadi N. Arthroscopy. 1999 Jul-Aug;15(5):507-14. • Compare effectiveness of traditional treatment vs. immediate arthroscopic stabilization in young patients with first traumatic anterior dislocation of the shoulder • Prospective, randomized, blinded trial • 40 skeletally mature patients < 30 yr • 20 pts, Immobilization for 3 wks + rehabilitation (group T) • 20 pts, Arthroscopic stabilization (< 4 weeks of injury) + immobilization/rehabilitation (group S) • 2 yr follow-up • Rate of redislocation: T = 47%, S = 15.9%, P = .03 • Western Ontario Shoulder Instability (WOSI) index showed significantly better results in the surgically treated group at the 33 months • T = 633.93 v S = 287.1, P = .03 • No significant difference in range of motion
Role of Arthroscopic Lavage? Wintzell et. Al. J Shoulder Elbow Surg. 1999 Sep-Oct;8(5):399-402. • Prospective randomized study, Sweden • Compared treatment results of arthroscopic lavage with results of conventional nonoperative treatment • 30 consecutive patients, traumatic primary anterior shoulder dislocation, 18-30 y, no history of shoulder problems • 2-year follow-up • 3 (20%) of 15 patients in the lavage group had a redislocated shoulder • 9 (60%) of 15 patients in the non-operative group (P = .03) • 2 in lavage group vs. 6 in control group had been operated on or were scheduled for stabilizing surgery • Functional outcome/Constant and Rowe shoulder scores did not reveal any significant difference (P = .07) • Joint effusion decreased more rapidly (33%) in arthroscopic lavage group vs. non-operated group
Indications for Surgery • 1) initial dislocation in a patient who participates in high-risk or high-demand activities in whom recurrent dislocation would be inopportune or dangerous • professional athletes, mountain climbers, certain types of construction workers • 2) recurrence of dislocation or subluxation after trauma treated adequately with nonoperative measures • 3) pain due to recurrent transient shoulder subluxation when the arm is used for overhead activities Gill & Zarins. Am J Sports Med, Jan-Feb, 2003.
Algorithm for Anterior Shoulder Instability J Am Acad Orthop Surg 1997;5:233-239
Nonanatomic Repairs • Bristow • Transfer coracoid process to anteroinferior glenoid • Sling effect and bone block • Putti-Platt • “Pants-over-vest” repair capsule • Magnusen-Stack • subscapularis tendon is detached from its insertion on the lesser tuberosity, transferred laterally to the greater tuberosity • Infrequent indications for using these procedures except in revision surgery
Anatomic Repairs • Restoring normal anatomy is guiding principle in surgery to correct anterior shoulder instability • If the labrum has been detached, it is reattached to the anterior glenoid rim • If the capsule has been stripped off the glenoid neck, the capsule is reattached to the bony glenoid rim • If greater than one-third of the glenoid fossa is involved, a bone block procedure such as a Bristow or iliac crest bone graft may be considered • Guidelines • Anatomic dissection at time of surgery • Identification and repair of lesions responsible for instability • Returning tissues to their anatomic locations • Early postoperative range of motion
Surgical Issues • Incision subscapularis tendon/capsule • Bankart repair • Capsular shift
Complications • Recurrent instability (10%) - most common causes • continued presence of avulsed anterior capsule and labrum from glenoid rim (unrepaired Bankart lesion) • excessive capsular laxity • an enlarged "rotator interval” • failure to diagnose correct direction(s) of instability • Other causes include • presence of a Hill-Sachs lesion • reduced humeral head retroversion • excessive glenoid cavity retroversion • avulsion of the anterior capsule from its lateral humeral attachment • scarred or weakened subscapularis muscle or tendon. • Neurovascular injury – musculocutaneous, axillary • Limitation of motion • Problems from retained hardware • Degenerative arthritis
Summary • Balance between the restoration of joint stability while minimizing loss of glenohumeral motion • Choice of treatment should be individualized • patient's occupation, level of participation in sports, degree of instability of the shoulder • No single "essential lesion" as proposed by Bankart • Bankart lesion is by far the most important • Open stabilization remains the standard procedure for treatment of anterior stabilization • esp. for severe instabilities, revision procedures, athletes in contact sports • Follow “anatomic repair principles”
Case • 25-year-old former collegiate football player presenting with 20 recurrent dislocations over the last 5 years
History • 25-year-old, right-hand-dominant, former collegiate football player • Suffered his first traumatic left shoulder dislocation at age 16 • He had an emergency room assisted reduction and was placed in a sling for 3 weeks • Underwent physical therapy for 2 months but subsequently had recurrent instability after returning to football • Age18, he underwent an arthroscopic Bankart reconstruction with 3 metal suture anchors • He began playing collegiate football, suffered a recurrent dislocation, and eventually had to discontinue playing • He has now had 20 recurrent dislocations over the last 5 years and presents for evaluation and treatment
Physical Examination • Active Shoulder Range of Motion: • Forward elevation180° bilaterally • ER (side) 60° bilaterally • ER (abduction) 90° bilaterally • IR T-7 spinous process bilaterally • Right Shoulder Instability Exam • Anterior load and shift 2+ • Posterior load and shift 1+ • Sulcus 1+ • Negative apprehension, relocation, anterior release • Left Shoulder Instability Examination: • Anterior load and shift 3+ • Posterior load and shift 1+ • Sulcus 1+ • No signs of generalized ligamentous laxity. • Positive apprehension, relocation, anterior release. • Normal neurological examination.
Imaging • Radiographs demonstrate a small Hill-Sachs lesion (yellow arrow) and the previously placed metal suture anchors (blue arrow).
Open anteroinferior capsular shift and Bankart procedure. • Modified beach chair position with the head elevated ~30° • Deltopectoral incision was used • Subscapularis was dissected off the underlying capsule
Bankart lesion • Capsule dissected off the humerus • Fukuda retractor placed to expose the glenohumeral joint • Large Bankart lesion was identified from the 6-9 o'clock position • Bioabsorbable suture anchors were used but had to be redirected carefully to avoid the previously placed metal suture anchors in the anteroinferior glenoid
Capsular Shift • Superolateral capsular shift (formal "T" capsulorrhaphy was not necessary) of the entire capsule • Arm placed in 30° abduction and 30° external rotation for capsular repair
Subscapularis Repair • Subscapularis was then anatomically repaired with #2 nonabsorbable sutures