Download
1 / 41
410 likes | 523 Vues
AFTERNOON DELIGHT obtaining and analyzing the fluid on your coat. Pathophysiology Review October 14th, 2010. Case.

E N D
AFTERNOON DELIGHTobtaining and analyzing the fluid on your coat Pathophysiology Review October 14th, 2010
Case A 72-year-old man with a history of hepatitis C cirrhosis, hepatocellular carcinoma, and migraine headaches is evaluated in the emergency department for a 24-hour history of altered mental status and fever. The patient complained to family members of general malaise and concern that he had a migraine “coming on.” His medical history also includes a portal vein thrombosus believed to be secondary to malignant hypercoagulability. On physical examination, the temperature is 38.2 °C, the blood pressure is 110/60 mm Hg, the pulse rate is 120/min, the respiration rate is 24/min, and the BMI is 30. Oxygen saturation is 95% with the patient breathing ambient air. Cardiac examination shows tachycardia and an S4. Breath sounds are normal. Abdominal exam exhibits significant ascites. Serum creatinine concentration is 1.1 mg/dL (185.6 µmol/L). Chest radiograph is negative for infiltrates, but shows a right pleural effusion.
What happened? Diagnostic tests History Results Interpretation Assessment
Why? Diagnostic tests History Results Interpretation Assessment
What are possible causes of AMS? 4:45 pm • A 72-year-old man with a history of hepatitis C cirrhosis, hepatocellular carcinoma, and migraine headaches is evaluated in the emergency department for a 24-hour history of altered mental status and fever. The patient complained to family members of general malaise and concern that he had a migraine “coming on.” His medical history also includes a portal vein thrombosus believed to be secondary to malignant hypercoagulability. • On physical examination, the temperature is 38.2 °C, the blood pressure is 110/60 mm Hg, the pulse rate is 120/min, the respiration rate is 24/min, and the BMI is 30. Oxygen saturation is 95% with the patient breathing ambient air. Cardiac examination shows tachycardia and an S4. Breath sounds are normal. Abdominal exam exhibits significant ascites. Serum creatinine concentration is 1.1 mg/dL (185.6 µmol/L). Chest radiograph is negative for infiltrates, but shows a right pleural effusion. History
Why? Diagnostic tests History Results Interpretation Assessment
Sources of Infection 5:15 pm • Meningitis • Empyema • Spontaneous bacterial peritonitis Assessment
Sources of Infection 5:15 pm Assessment Meningitis Empyema Spontaneous bacterial peritonitis
Meningitis 5:15 pm • Inflammatory disease of the leptomeninges • Infection of the arachnoid mater and the CSF in both the subarachnoid space and the cerebral ventricles Assessment
Blood Brain Barrier (BBB) 5:15 pm Assessment • Cerebral capillary endothelium is responsible for the blood brain barrier • Unique from other systemic capillay beds • Cerebral capillary endothelium exhibit rare pinocytosis and the plasma membranes of adjacent endothelial cells are fused together in the form of continuous intact intercellular tight junctions • High mitochondrial density of the cerebral endothelium provides energy dependent transport of sodium and potassium at the antiluminal membrane • All these allow for homeostasis of the perineuronal interstitial fluid • Only lipid-soluble substances or those transported by carrier-mediated diffusion (glucose, essential amino acids) traverse the BBB normally • -
Alterations of the BBB 5:15 pm Assessment • Ednotoxins and related cytokine response results in the increased permeability of the BBB • From 4-18 hours, there is an increase in pinocytosis and sepearation of the intercellular tight junctions • Host defense mechanisms in the subarachnoid space are typically inadequate to control infections sources • Complement activity, although low, hypothetically serves to draw leukocytes across the BBB
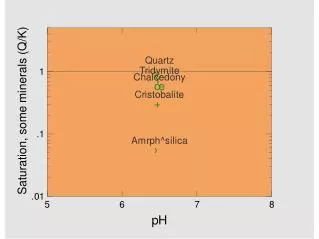
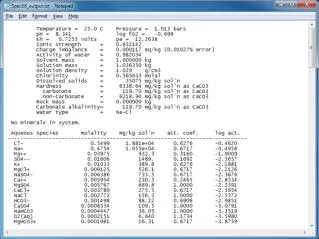
CSF Interpretation 9:10 pm • - • - Results Mason: Murray and Nadel's Textbook of Respiratory Medicine, 5th ed.
Sources of Infection 5:15 pm Assessment • Meningitis • Empyema • Sponteous bacterial peritonitis
Pleural Effusions • Influx and exit of liquid and protein of the pleural space are balanced so that a constant volume of protein concentration exists in the normal state • With changes in microvascular hydrostatic or oncotic pressure, pleural pressure, and microvascular permeability, or with impaired lymphatic drainage, this delicate balance is disturbed: fluid accumulates and protein concentration changes
Pleural Effusions • Pleural fluid should be considered as interstitial liquid of the parietal pleura • Since the parietal pleura is supplied by the systemic circulation and the pressure of the pleural space is subatmospheric and probably less than the pressure in the interstitium of the subpleural space, there is a pressure gradient from the pleural interstitium to the pleural space • The reserve of pleural lymphatics are large,and for a pleural effusion to form, fluid formation rate must be very high or lymphatic flow impaired
Pleural Effusion Formation • An increased rate of formation of pleural fluid can occur with: • increase in microvascular hydrostatic pressure, • decrease in microvascular oncotic pressure • decrease in pressure in the pleural space, and increase in microvascular permeability • movement of fluid from the peritoneal to the pleural space
Empyema • Empyema is pus in the pleural space • Typically end of continuum of parapneumonic effusion • Exudative • pH less than 7.0
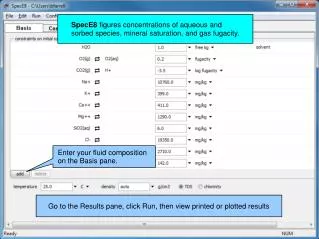
Thoracentesis results 9:10 pm Results
Sources of Infection 5:15 pm Assessment Meningitis Empyema Spontaneous bacterial peritonitis
Ascites • The accumulation of ascitic fluid represents a state of total-body sodium and water excess • The underfilling theory suggests that the primary abnormality is inappropriate sequestration of fluid within the splanchnic vascular bed due to portal hypertension and a consequent decrease in effective circulating blood volume. This activates the plasma renin, aldosterone, and sympathetic nervous system, resulting in renal sodium and water retention • The overflow theory suggests that the primary abnormality is inappropriate renal retention of sodium and water in the absence of volume depletion. This theory was developed in accordance with the observation that patients with cirrhosis have intravascular hypervolemia rather than hypovolemia • The peripheral arterial vasodilatino theory suggests that portal hypertension leads to vasodilation, which causes decreased effective arterial blood volume. As the natural history of the disease progresses, neurohumoral excitation increases, more renal sodium is retained, and plasma volume expands. This leads to overflow of fluid into the peritoneal cavity. The vasodilation theory proposes that underfilling is operative early and overflow is operative late in the natural history of cirrhosis
Spontaneous Bacterial Peritonitis • Spontaneous bacterial peritonitis (SBP) is defined as an ascitic fluid infection without an evident intraabdominal surgically-treatable source • Gram-negative microorganisms of intestinal origin are among the most frequent causes of infection in cirrhosis • The main mechanism underlying the development of SBP, as well as other bacterial infections in cirrhosis, is represented by bacterial translocation from the intestinal lumen to mesenteric lymph nodes or other extraintestinal organs and sites. • This process is facilitated by several factors, including changes in intestinal flora, portal hypertension, and, mainly, impairment in local/systemic immune defense mechanisms. • The diagnosis is established by a positive ascitic fluid bacterial culture and an elevated ascitic fluid absolute polymorphonuclear leukocyte (PMN) count (≥250 cells/mm3)
Serum-Ascites Albumin Gradient (SAAG) • Helps discriminate transudative ascites versus exudative ascites • The SAAG is calculated by subtracting the ascitic fluid albumin value from the serum albumin value, which is obtained on the same day • The presence of a gradient greater than 1.1 g/dL (11 g/L) indicates that the patient has portal hypertension with 97 percent accuracy (transudative ascites) • The presence of a gradient less than 1.1 g/dL (11 g/L) indicates that the patient does not have portal hypertension (exudative ascites)
Ascitic Fluid 9:10 pm • - • - Results
Interpretation • Patient diagnosed with spontaneous bacterial peritonitis • Started on ceftriaxone for culture positive E. Coli • Mental status recovered • Discharged 5 days later