Download
1 / 48
540 likes | 859 Vues
Evidenced Based Management Knee Osteoarthritis. Dr Jonathan Mulford myorthopod.com.au. Knee Arthritis. The reality - not life threatening and has low associated mortality. However- substantial influence on the quality of life heavy economic burden on the community. .

E N D
Evidenced Based Management Knee Osteoarthritis Dr Jonathan Mulford myorthopod.com.au
Knee Arthritis • The reality - not life threatening and has low associated mortality. • However- • substantial influence on the quality of life • heavy economic burden on the community.
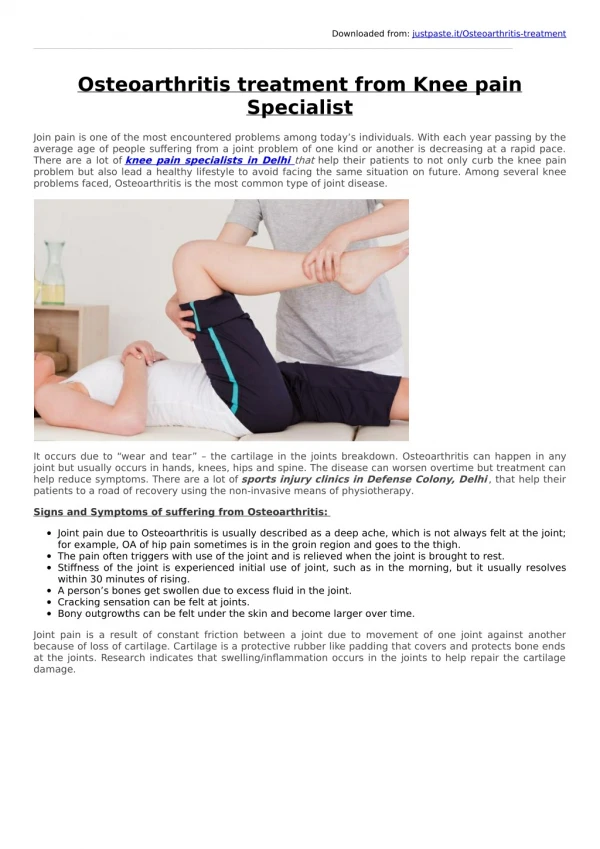
Risk factors for knee osteoarthritis • female • aging • Overweight • joint injury, malalignment, joint laxity, • occupational and recreational use • family history • Heberden's nodes at the distal finger joints.
Non Operative Management • Many Controversial treatments. • Many of this evidence Based finding are from the Cochrane Library • Unfortunately there are many studies of poor methodology.
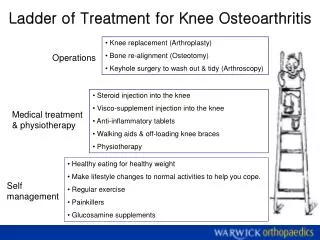
Non Op Treatments Groups • Lifestyle modification • Rehabilitation and Physiotherapy • Braces and Insoles • Pharmacology
LIFE STYLE MODIFICATION • Avoid aggravating factors • No high Impact • Limit Stair climbing • Weight loss • Diet
Weight loss and Knee OA • moderate weight loss (weight reduction > 5.1% or > 0.24%/wk) improves self-reported disability. • No clear evidence that Weight loss reduces pain or improve patient global evaluation. • A BMI greater than 30 has a 4 times increase in risk of knee arthritis – so weight loss important preventative measure!
Diet • A diet high in olive oil, fish and vegetables • reduced pain by 40% & morning stiffness by 10% in RA. • ? effects for OA. Annals of the Rheumatic Diseases 2003; 62:208-14. • Diets rich in vitamins C slow the progression of osteoarthritis. Arthritis and Rheumatism 1996; 39:648-56. .
REHABILITATION • Therapeutic Excercise • Ultrasound, TENS, Pulsed Electric Stimulation, Acupuncture • Hydrotherapy • Aquatic Excercise • Balneotherapy
Therapeutic Exercise in Knee OA • Small short term benefit for knee pain and physical function. • No evidence long term benefit. • Is useful pre-operatively.
Aquatic-exercise and Knee OA • some beneficial short-term effects for patients with hip and/or knee OA. • no long-term effects have been documented. • Can be useful for pre-operative conditioning.
Balneotherapy (or spa therapy, mineral baths) • The scientific evidence is weak. • Cochrane review - Seven trials (498 patients) • mineral baths compared to no treatment • Dead Sea + sulphur versus no treatment, • Dead Sea baths versus no treatment • sulphur baths versus no treatment • mineral baths may be benificial (small effect). • Of all other balneological treatments no clear effects were found.
Therapeutic ultrasound • no benefit over placebo
Transcutaneous electrical nerve stimulation (TENS) • small improvements in pain control over placebo. • Methodology of the studies is poor.
Pulsed Electric Stimulation • Electrical stimulation therapy had a small to moderate effect on outcomes for knee OA.
Acupuncture • randomised controlled trial”, Foster et al. (BMJ 2007;335;436), • acupuncture no benefit as an adjunct to a course of individualised, exercise based physiotherapy. • Other papers looking at acupuncture - some benefit • however have had major methodological flaws . • Annals of Internal Medicine 2004; 141(12):901-10.
Thermotherapy and knee OA • Ice massage beneficial effect on ROM, swelling, function and knee strength. • Ice packs did not affect pain significantly. • Hot packs had no beneficial effect on edema compared with placebo or cold application.
Brace and Orthosis (insole). • Brace (neoprene sleeve) and a lateral wedge insole have small beneficial effect. • However, long-term adherence to brace and insole treatment is low.
Pharmacology • Painkillers • Anti-inflammatory • Chondrotin and Glucosamine • Alternative medications • Injections
Paracetamol versus Placebo and versus NSAIDs • significant reduction in pain compared to placebo • BUT • Small improvements in pain. • less effective overall than NSAIDs in terms of pain reduction, global assessments and in terms of improvements in functional status.
NSAIDS • NSAIDs are effective in relieving short-term pain in OA. • NSAIDs at the lowest effective dose should be considered in patients who respond inadequately to simple analgesia. • longer-term use is potential for serious side effects.(gastropathy, including peptic ulcer disease, and care if hypertension, cardiovascular and renal disease) • Concurrent use of more than one NSAID and other medications, increasing age and duration of treatment substantially increase the risk of side effects.
Topical NSAIDS • Topical NSAIDs were effective and safe in short-term treatment of OA. • lack of any trial data to support their long-term use • Effects wane after 2 weeks. • Larger and longer trials are necessary
COX-2 • CLASS study demonstrated that coxibs reduce clinical upper GI events by approximately 55% • Consider COX-2 if high risk of peptic ulcer disease. • Caution should be used due to their association with cardiovascular, renal and other adverse effects.
Opioid Analgesia • alternative when paracetamol and NSAID drugs are contraindicated, ineffective, or poorly tolerated. • A once-a-day formulation of tramadol helps pain, • fewer interruptions in sleep and improved compliance. • effective alternative treatment for acute flares of OA pain.
CODEINE • Codeine in combination with simple analgesia or NSAID might be appropriate for the occasional pain relief or for patients in whom only simple analgesia is not effective. • However, repeated use increases the occurrence of side effects.
Chondroitin • 22 RCTs (n = 4056) • Conclusion: Based on evidence from higher-quality trials of patients with knee or hip osteoarthritis, chondroitin does not reduce pain more than placebo or no treatment.
Glucosamine • 25 studies with 4963 patients. • If Analysis restricted to studies with adequate allocation concealment • No benefit for pain, function and stiffness subscales. • Collectively, the 25 RCTs • 22% (improvement in pain and a 11% improvement in function • Non-Rotta preparation or adequate allocation concealment failed to show benefit in pain and WOMAC function • Rotta preparation showed that glucosamine was superior to placebo in the treatment of pain and functional impairment resulting from symptomatic OA.
Alternative Herbal Medicine • Cochrane review found 5 studies. • The evidence for avocado-soybean unsaponifiablesin the treatment of osteoarthritis is convincing . • Single studies of other interventions, a willow bark preparation (Reumalex), topical capsaicin and tipi tea, were inconclusive.
Corticosteroid Injections • Effective pain reliever however often only for short period (4 weeks)
Viscosupplements • at one to four weeks post injection CSI and HA same. • Between five and 13 weeks post injection, HA products were more effective than corticosteroids
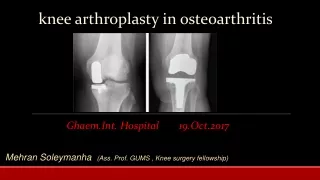
Surgical Treatment • Arthroscopy • Osteotomy • Uni • Patellofemoral Arthroplasty • Total knee Arthroplasty • Fusion
Arthroscopic Surgery • There is 'gold' level evidence that AD has no benefit for undiscriminated OA • Can help acute mechanical pain due to meniscal tear, chondral flap or loose body. • The acute pain is helped, however can have residual pain from the OA.
High Tibial Osteotomy Indications • Isolated Compartment OA • Less than 12 degrees deformity • Stable knee • Young and active Benefits • Avoid arthroplasty • No limits on activity
Problem • Inconsistent results – 50% still effective at 7-10 years • At 5 years 75% good or excellent. • At 8 years 60% good or excellent. • (Arch Orthop Trauma Surg 124:258-261, 2004) • Arthroplasty after osteotomy may not be as successful. • Certainly more challenging surgery.
Uni Indications • isolated compartment Osteoarthritis. Benefits • Smaller incision, Quicker recovery, better feeling knee, cost implications. Problems • progression, revision.
How Long do they Last? • Swedish Register – about 90% at 10 years
Patellofemoral Arthroplasty • Indications – Isolated • Benefits • Problems
When to Operate • When pain is bad enough to limit lifestyle and function. • Don’t wait too long - • surgery performed later in the natural history of functional decline results in worse postoperative functional status. • However, • those with the poorest preoperative scores gained most from the operation. • patients operated on later were more satisfied with their outcomes.
Total knee Replacement • 91-96% prosthesis survival rate at 14-15 years of follow-up. • We now know that approximately 85 percent of the knee implants will last 20 years. • Thus most implants will last a life time.
Improvements in surgical technique, prosthetic designs, bearing surfaces, and fixation methods might increase the survival rate of these implants even longer.
Revision Summary Australian Joint Register • At 7 years cumulative % revision • Primary total 4.3% • Uni 12.1% • PFJ 13.8%