Download
1 / 70
1.6k likes | 5.72k Vues
Double Filtration Plasmapheresis (DFPP). 賴俊夫醫師 台大醫院內科部腎臟科 台大醫院急性腎衰竭研究群 NSARF Renal Division, Department of Internal Medicine, National Taiwan University Hospital NTUH Study group on Acute Renal Failure. Plasma therapy in CVS (TPE, DFPP, ECP). 賴俊夫醫師 內科部腎臟科. March 25, 2011. 血漿治療.

E N D
Double Filtration Plasmapheresis (DFPP) 賴俊夫醫師 台大醫院內科部腎臟科 台大醫院急性腎衰竭研究群NSARF Renal Division, Department of Internal Medicine, National Taiwan University Hospital NTUH Study group on Acute Renal Failure
Plasma therapy in CVS (TPE, DFPP, ECP) 賴俊夫醫師 內科部腎臟科 March 25, 2011
血漿治療 • Plasma – 血漿 • Apheresis – 分離; Exchange – 交換 • 血漿分離術 (Plasmapheresis) • 將血液中血球與血漿分離,以移除血漿中較大分子量的有害成份 • 血漿置換術 (Plasma exchange) • 將血漿取出體外,去除血漿中的有害物質,再換以正常人的血漿。
Molecular weight of removed substances by blood purification therapy
離心式血漿分離 補充液
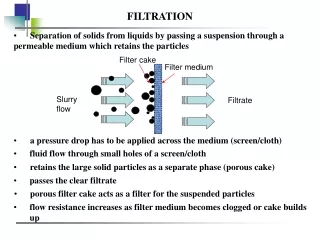
空心纖維膜血漿分離 • 治療性血漿交換術 (TPE, Therapeutic Plasma Exchange) • 輸注他人血漿,以補充移除的血漿 • 雙重血漿分離術 (DFPP, Double Filtration Plasmapheresis) • 利用兩個人工腎臟,減少移除的血漿量
空心纖維膜血漿分離 補充液 補充液 FFP, Plasmanate, Lacted Ringer’s
PlasmacureTM (ASAHI KURARAY MEDICAL CO., LTD) Plasma seperator
雙重過濾血漿分離術 補充液 N/S 0.03μm 0.2μm 去除血漿中有害成分(分離血漿的10%,約血流的3%)
血漿移除量 1 plasma voulem = BW X (1/13) X (1-Hct) Plasma volume Volume exchanged Immunoglobulin exchange( Ve/EPV ) ( Ve, ml ) or other substance removed (MRR,%) eg. 60kg, Hct 40% 0.5 1,400 39 1.0 2,800 63 1.5 4,200 78 2.0 5,600 86 2.5 7,000 92 3.0 8,400 95
血漿補充量 • 視血漿移除量多寡 • Plasma exchange • 移除2 plasma volume 5600 cc 血漿 • 22U FFP + 5 plasmanate + 3 Ringer’s • Double filtration plasmapheresis移除量 • 移除1.5 plasma volume 4200 cc 血漿血漿量x10% = 420cc • 3U FFP, or 500cc Ringer’s, or albumin
治療機轉 • 血漿移除 • 血漿輸注
可能的治療機轉血漿移除 • 移除血漿中可能的致病因子: TPE, DFPP • Antibodies (Anti-GBM Ab disease; MG) • Immune complex (SLE) • Cryoglobulin (Cryoglobulinemia) • Myeloma protein (Myeloma nephropathy( • Endotoxin, cytokine (Sepsis) • Poison or drug • Cholesterol, LDL-c
可能的治療機轉血漿輸注 • 補充血中缺乏之因子: TPE only • Anti-thrombotic or fibrinolytic factor (HUS/TTP): removal of auto-antibodies to vWF multimers cleaving enzyme + infusion of vWF multimers cleaving enzyme • 免疫調控 (Immunomodulation) • Removal of complement products (SLE) • Effect of immune regulation (Transplantation) • Improvement in RE function (cyroglobulinemia)
健保給付之適應症 • 58008C血漿置換術(2475點) Plasma exchange:限下列病患實施 • 1.SLE,CNS involvement • 2.Myasthenia gravis crisis • 3.Macroglobulinaemia • 4.RPGN • 5.Goodpasture's disease • 6.Multiple myoloma • 7.Guillain-Barre syndrome • 8.Thrombocytopenic Purpura • 9.其他經專案向保險人申請同意實施者 • 58016C二重過濾血漿置換療法(2475點) Double filtration plasmapheresis:施行本項之適應症請依支付標準58008C「血漿置換術」之規定辦理。
ASFA guidelines e.g. SLE lupus nephritis
Traffic Accident Transfer to NTUH Desaturation PCWP 40 mmHg Dilate LV Cardiac echo: LVEF 19% Extubation 8/14 8/15 8/16 8/23 8/31 9/1 9/5 9/6 9/15 10/5 10/20 VV-ECMO LV Drain LV Assist Device LM dissection s/p POBAS Cardiac cath: No ISRS Remove VV-ECMO
Transplantation Panel reactive antibody: Anti-HLA class I: 61% Anti-HLA class II: 72%
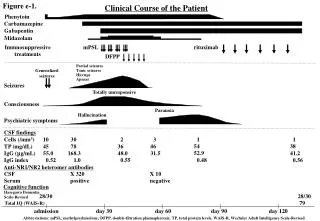
11/4 11/6 11/8 11/10 11/12 Double Filtration Plasmapheresis 3L/session, 1.2x plasma volume total 5 course Rituximab (Mabthera) 200 mg Bortezomib (Velcade) 3.5 mg Solu-Medrol 1000 mg Intravenous immunoglobulin 45 gm R-anti-thymocyte globulin 25 mg Plasma Exchange Hypotension, Bradycardia 11/3 Donor
Isoproterenol Millisrol Dopamine Primacor (Milrinone) Bosmin 3000 Graft failure ? 2500 CO: 2.23 CI: 1.48 2000 1500 1000 CVVH 500 11/11 11/12 11/13 11/14 11/15 11/16 11/17 11/18 11/19 Massive bloody pleural effusion Transplant DFPP DFPP IVIG IVIG Solu-Medrol FK506 Cellcept
Sensitization • Blood transfusions • Pregnancy • Previous organ transplant • Placement of a ventricular device Approximate 30% incidence of antibody production (PRA > 10%) after LVAD placement J Heart Lung Transplant 2002; 21: 1218-24 • Definition • Exposure of the immune system to antigen (transplant organ) sufficient to generate an immune response • Antibody • ABO • Anti-HLA • Non-HLA
Prevent rejection Humoral Response Cellular Response Donor selection Immunosuppressive agents Recipient Desensitization
Examples of desensitization J Heart Lung Transplant 2009;28:213-25
Pre-heart transplant plasmaheresis for sensitized patients (high PRA) • 1.5 plasma volume plasmapheresis + 20g 5% IVIG, then heart transplant • 1.5 plasma volume plasmapheresis qod (followed by 20g 5% IVIG )X 5 sessions. Then a single plasmaphereis with IVIG at the time of surgery J Heart Lung Transplant 1999;18:701 Clin Transplant 2006;20:476-84
HLA class I HLA class II Clin Transplant 2006;20:476-84 Clin Transplant 2006: 20: 476–484
On-pump TPE for XM heart transplant • High blood flow and thus increased pheresis rate to shorten treatment time than standard setting of TPE/DFPP • 3 plasma volume within 60-90min • Especially need to watch out [Ca] J Extra Corpor Technol 1999;31:177-83 J Heart Lung Transplant 2008;27:1036-9
Comparative long-term outcome 5-year patient survival 1-year rejection-free survival 523 heart transplant, 95 PRA>10%, 21/95 desensitization, 74 untreated Survival: no significant difference Rejection: significant decrease in desensitized patients (Treated with PP+IVIG+Rituximab) Clin Transplant. 2010 Oct 25
Proposed protocol for desensitization Solumedrol 500mg IVIG 15g (heart lung machine) Bortezomib (Velcade) IV slow push IVIG 30g slowing infusion Solumedrol 500mg + Rituximab (Mabthera) IV drip RATG + FK506 D-9 D-7 D-5 D-3 D-1 OP day D1 D3 D5 TIW 1.5 PV DFPP 1.5 PV DFPP 1.5 PV DFPP 1.5 PV DFPP 1.5 PV DFPP 1.5 PV DFPP 1.5 PV DFPP 1.5 PV DFPP 1.5 PV DFPP 2 PV TPE (OR) IVIG IVIG IVIG IVIG IVIG Initial Ab X(1-78%)5 =0.0005 initial amount residual Ab X(1-86%)
Extracorporeal photopheresis T-cell B-Cell
Primary prophylaxis Clin Transplantation 2000;14:162-6 N Engl J Med 1998;339:1744-51
Secondary prophylaxis J Heart Lung Transplant 2006;25:283-8
Extracorporeal photopheresis (ECP) • Leukapheresis-based immunomodulatory therapy. • Mechanism: • causes apoptosis of the treated and abnormal T cells • induces monocytes to differentiate into dendritic cells capable of phagocytosing and processing the apoptotic T-cell antigens • may cause a systemic cytotoxic CD8+ T-lymphocyte–mediated immune response to the processed apoptotic T-cell antigens • induce antigen-specific regulatory T cells, which may lead to suppression of allograft rejection or GVHD
ECP Procedures • 3 basic stages: (1) leukapheresis, (2) photoactivation, and (3) reinfusion. The process takes 3-4 hours to complete. • Blood (225 mL) is passed through 3 cycles of leukapheresis, or 125 mL of blood is passed through 6 cycles, depending on the patient's hematocrit value and body size. At the end of each leukapheresis cycle, the red blood cells and plasma are returned to the patient. • The collected WBCs (including approximately 5% of the peripheral blood mononuclear cells) are mixed with heparin, saline, and 8-methoxypsoralen (8-MOP), which intercalates into the DNA of the lymphocytes upon exposure to UVA light and makes them more susceptible to apoptosis when exposed to UVA radiation. • The mixture is passed as a 1-mm film through a sterile cassette surrounded by UVA bulbs for 180 minutes, resulting in an average UVA exposure of 2 J/cm2 per lymphocyte. • The treated WBC mixture is returned to the patient.
ECP Complications • Hypotension may occur in some patients during the collection phase of the treatment. • Low-grade fevers, likely due to the release of cytokines. • Some patients with cutaneous T-cell lymphoma (CTCL) may experience an increase in pruritus or redness. • No immunosuppression, opportunistic infections, or neoplasia has been associated with extracorporeal photopheresis.
Acute AMR after heart transplant Anti-B-memory and/or plasma cells agents Am J Transplant 2007;7:2064-74 Transplant Rev 2009;23:34-46
血漿分離術之併發症 • 血管通路 • 血胸、氣胸、後腹腔出血 • 抗凝劑 • 出血 • Hypothermia • Hyperthermia blanket , Warm lamp, Warmer