Download
1 / 18
180 likes | 644 Vues
Health care-associated pneumonia (HCAP). Definitions Hospital-acquired pneumonia or nosocomial pneumonia (HAP) refers to a newepisode of pneumonia occurring at least 2 days after admission to hospital. It is the second most common hospital-acquired infection (HAI).

E N D
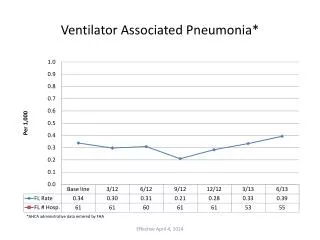
Definitions Hospital-acquired pneumonia or nosocomial pneumonia (HAP) refers to a newepisode of pneumonia occurring at least 2 days after admission to hospital. • It is the second most common hospital-acquired infection (HAI). • Older people are particularly at risk, also at risk are patients in intensive care units, especially when mechanically ventilated, in which case the term ventilator-associated pneumonia (VAP) is applied. Health care-associated pneumonia (HCAP) refers to the • Development of pneumonia in a person who has spent at least 2 days in hospital within the last 90 days, • Attended a haemodialysis unit, • Received intravenous antibiotics, • Or been resident in a nursing home or other long-term care facility.
Aetiology Of hospital acquired pneumonia
Factors predisposing to hospital-acquired pneumonia Reduced host defences against bacteria • Reduced immune defences (e.g. corticosteroid treatment, diabetes, malignancy) • Reduced cough reflex (e.g. post-operative) • Disordered mucociliary clearance (e.g. anaesthetic agents) • Bulbar or vocal cord palsy Aspiration of nasopharyngeal or gastric secretions • Immobility or reduced conscious level • Vomiting, dysphagia, achalasia or severe reflux • Nasogastric intubation Bacteria introduced into lower respiratory tract • Endotracheal intubation/tracheostomy • Infected ventilators/nebulisers/bronchoscopes • Dental or sinus infection Bacteraemia • Abdominal sepsis • I.v. cannula infection • Infected emboli
Clinical features and investigations • HAP should be considered in any hospitalised or ventilated patient who develops: • purulent sputum (or endotracheal secretions), • new radiological infiltrates, • an otherwise unexplained increase in oxygen requirement, • a core temperature > 38.3°C, • and a leucocytosis or leucopenia. • Appropriate investigations are similar to those outlined for CAP, In mechanically ventilated patients, • bronchoscopy-directed protected brush specimens • or bronchoalveolarlavage (BAL) may be performed. • Endotracheal aspirates are easy to obtain but less reliable.
Management • Adequate Gram-negative cover is usually provided by: a third-generation cephalosporin (e.g. cefotaxime) with an aminoglycoside (e.g. gentamicin), meropenem or a monocyclic β-lactam (e.g. aztreonam) • and flucloxacillin. • MRSA is treated with intravenous vancomycin. • The nature and severity of most HAPs dictate that these antibiotics are all given intravenously. • Physiotherapy is important in those who are immobile or old. • Adequate oxygen therapy, • Fluid support and monitoring are essential.
Prevention • Despite appropriate management, the mortality from HAP is high at approximately 30%, emphasising the importance of prevention. • Good hygiene is paramount, including both hand washing and equipment. • Steps should be taken to minimise the chances of aspiration and limit the use of stress ulcer prophylaxis with proton pump inhibitors. • Oral antiseptic (chlorhexidine 2%) may be used to decontaminate the upper airway and some intensive care units use selective decontamination of the digestive tract when the anticipated requirement for ventilation will exceed 48 hours.
These conditions are considered together, as their aetiology and clinical features overlap. • Suppurative pneumonia is characterised by destruction of the lung parenchyma by the inflammatory process; • Although microabscess formation is a characteristic histological feature, 'pulmonary abscess' is usually taken to refer to lesions in which there is a large localised collection of pus, or a cavity lined by chronic inflammatory tissue, from which pus has escaped by rupture into a bronchus.
Risk factors and Aetiology • Suppurative pneumonia and pulmonary abscess often develop after the inhalation of septic material during operations under general anaesthesia, or of vomitusduring anaesthesia or coma, particularly if oral hygiene is poor. • Additional risk factors for aspiration pneumonia include bulbar or vocal cord palsy, stroke, achalasia or oesophageal reflux, and alcoholism. • Aspiration tends to localise to dependent areas of the lung such as the apical segment of the lower lobe in a supine patient. Depending on patient’s position during inhalation. • Suppurative pneumonia and abscess may also complicate local bronchial obstruction from a neoplasm or foreign body.
Microbiology • Infections are usually due to a mixture of anaerobes and aerobes in common with the typical flora encountered in the mouth and upper respiratory tract, and isolates of Bacteroides, Fusobacteriumnecrophorum, anaerobic or microaerophiliccocci may be identified. • When suppurative pneumonia or pulmonary abscess occurs in a previously healthy lung, the most likely infecting organisms are Staph. aureus or Klebsiellapneumoniae. • In many cases, however, no pathogen can be isolated, particularly when antibiotics have been given. • Recently, cases of community-acquired MRSA (CA-MRSA) have been reported. This organism is distinct from MRSA but produces the toxin Panton-Valentine leukocidin, which causes a rapidly progressive severe necrotising pneumonia. • Injecting drug-users are at particular risk of developing haematogenous lung abscess, often in association with endocarditis affecting the pulmonary and tricuspid valves.
Clinical features of suppurative pneumonia Symptoms • Cough productive of large amounts of sputum which is sometimes fetid and blood-stained • Pleural pain common • Sudden expectoration of copious amounts of foul sputum occurs if abscess ruptures into a bronchus Clinical signs • High remittent pyrexia • Profound systemic upset • Digital clubbing may develop quickly (10-14 days) • Chest examination usually reveals signs of consolidation; signs of cavitation rarely found • Pleural rub common • Rapid deterioration in general health with marked weight loss can occur if disease not adequately treated Investigations • Radiological features of suppurative pneumonia include homogeneous lobar or segmental opacity consistent with consolidation or collapse. • Abscesses are characterised by cavitation and fluid level. • Occasionally, a pre-existing emphysematous bulla becomes infected and appears as a cavity containing an air-fluid level. • CT scan of the chest is sometimes needed. • Sputum and blood should be sent for culture.
Management • Aspiration pneumonia can be treated with iv co-amoxiclav . If an anaerobic bacterial infection is suspected (e.g. from fetor of the sputum), oral metronidazole should be added. • Further modification of antibiotics should be informed by clinical response and the microbiological results. • CA-MRSA is usually susceptible to a variety of oral non-β-lactam antibiotics, such as trimethoprim/sulfamethoxazole, clindamycin, tetracyclines and linezolid. Parenteral therapy with vancomycin or daptomycin can also be considered • Prolonged treatment for 4-6 weeks may be required in some patients with lung abscess. • Physiotherapy is of great value, especially when suppuration is present in the lower lobes or when a large abscess cavity has formed. • In most patients, there is a good response to treatment, and although residual fibrosis and bronchiectasis are common sequelae, these seldom give rise to serious morbidity. • Surgery should be contemplated if no improvement occurs despite optimal medical therapy. Removal or treatment of any obstructing endobronchial lesion is essential.
Pneumonia in the immunocompromised patient The majority of infections are caused by the same pathogens that cause pneumonia in non-immunocompromised individuals, But in patients with more profound immunosuppression, unusual organisms, or those normally considered to be of low virulence or non-pathogenic, may become 'opportunistic' pathogens. In addition to the more common agents, the possibility of Gram-negative bacteria, especially Pseudomonas aeruginosa viral agents, fungi, mycobacteria, and less common organisms such as Nocardiaasteroides.
Clinical features • These typically include fever, cough and breathlessness, • In general, the onset of symptoms tends to be less rapid when caused by opportunistic organisms such as Pneumocystisjirovecii and in mycobacterial infections, than with bacterial infections . • In P. jirovecii pneumonia, symptoms of cough and breathlessness can be present several days or weeks before the onset of systemic symptoms or the appearance of radiographic abnormality. Diagnosis • Invasive investigations such as bronchoscopy, or surgical lung biopsy are often impractical, as many patients are too ill to undergo these safely. • However, 'induced sputum' may offer a relatively safe method of obtaining microbiological samples. • HRCT is useful in differentiating the likely cause: • Focal unilateral airspace opacificationfavours bacterial infection, mycobacteria or nocardia. • Bilateral opacificationfavoursP. jirovecii pneumonia, fungi and viruses . • Cavitation may be seen with mycobacteria and fungi. • The presence of a 'halo sign' may suggest Aspergillus . • Pleural effusions suggest a pyogenic bacterial infection.
Management • In practice, the causative agent is frequently unknown and broad-spectrum antibiotic therapy is required, such as: a third-generation cephalosporin, or a quinolone, plus an antistaphylococcal antibiotic, or • an antipseudomonal penicillin plus an aminoglycoside. • Thereafter treatment may be tailored according to the results of investigations and the clinical response. • Depending on the clinical context and response to treatment, antifungal or antiviral therapies may be added. • Mechanical ventilation increases the risk of nosocomial pneumonia and is associated with a greater mortality rate. It may be avoided by the early use of NIV. • The delivery of NIV via a hood is as effective as a face mask and allows the patient to expectorate, communicate and feed.