Download
1 / 1
20 likes | 138 Vues
No. 038. Informed consent in TURP: Should structured written consent form the minimum standard of practice within the 21 st century? ).

E N D
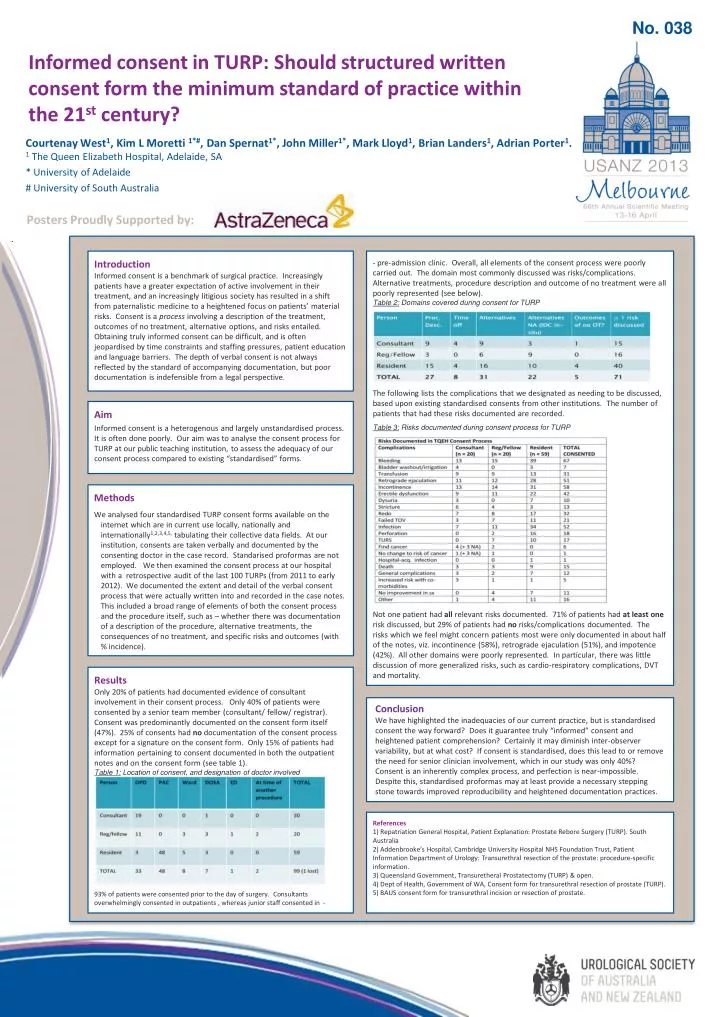
No. 038 Informed consent in TURP: Should structured written consent form the minimum standard of practice within the 21st century?) Courtenay West1, Kim L Moretti1*#,Dan Spernat1*, John Miller1*, Mark Lloyd1, Brian Landers1, Adrian Porter1. 1 The Queen Elizabeth Hospital, Adelaide, SA * University of Adelaide # University of South Australia Posters Proudly Supported by: Introduction Informed consent is a benchmark of surgical practice. Increasingly patients have a greater expectation of active involvement in their treatment, and an increasingly litigious society has resulted in a shift from paternalistic medicine to a heightened focus on patients’ material risks. Consent is a process involving a description of the treatment, outcomes of no treatment, alternative options, and risks entailed. Obtaining truly informed consent can be difficult, and is often jeopardised by time constraints and staffing pressures, patient education and language barriers. The depth of verbal consent is not always reflected by the standard of accompanying documentation, but poor documentation is indefensible from a legal perspective. - pre-admission clinic. Overall, all elements of the consent process were poorly carried out. The domain most commonly discussed was risks/complications. Alternative treatments, procedure description and outcome of no treatment were all poorly represented (see below). Table 2: Domains covered during consent for TURP The following lists the complications that we designated as needing to be discussed, based upon existing standardised consents from other institutions. The number of patients that had these risks documented are recorded. Table 3: Risks documented during consent process for TURP Not one patient had all relevant risks documented. 71% of patients had at least one risk discussed, but 29% of patients had no risks/complications documented. The risks which we feel might concern patients most were only documented in about half of the notes, viz. incontinence (58%), retrograde ejaculation (51%), and impotence (42%). All other domains were poorly represented. In particular, there was little discussion of more generalized risks, such as cardio-respiratory complications, DVT and mortality. Aim Informed consent is a heterogenous and largely unstandardised process. It is often done poorly. Our aim was to analyse the consent process for TURP at our public teaching institution, to assess the adequacy of our consent process compared to existing “standardised” forms. Methods We analysed four standardised TURP consent forms available on the internet which are in current use locally, nationally and internationally1,2,3,4,5, tabulating their collective data fields. At our institution, consents are taken verbally and documented by the consenting doctor in the case record. Standarisedproformas are not employed. We then examined the consent process at our hospital with a retrospective audit of the last 100 TURPs (from 2011 to early 2012). We documented the extent and detail of the verbal consent process that were actually written into and recorded in the case notes. This included a broad range of elements of both the consent process and the procedure itself, such as – whether there was documentation of a description of the procedure, alternative treatments, the consequences of no treatment, and specific risks and outcomes (with % incidence). Results Only 20% of patients had documented evidence of consultant involvement in their consent process. Only 40% of patients were consented by a senior team member (consultant/ fellow/ registrar). Consent was predominantly documented on the consent form itself (47%). 25% of consents had no documentation of the consent process except for a signature on the consent form. Only 15% of patients had information pertaining to consent documented in both the outpatient notes and on the consent form (see table 1). Table 1: Location of consent, and designation of doctor involved 93% of patients were consented prior to the day of surgery. Consultants overwhelmingly consented in outpatients , whereas junior staff consented in - Conclusion We have highlighted the inadequacies of our current practice, but is standardised consent the way forward? Does it guarantee truly “informed” consent and heightened patient comprehension? Certainly it may diminish inter-observer variability, but at what cost? If consent is standardised, does this lead to or remove the need for senior clinician involvement, which in our study was only 40%? Consent is an inherently complex process, and perfection is near-impossible. Despite this, standardisedproformas may at least provide a necessary stepping stone towards improved reproducibility and heightened documentation practices. References1) Repatriation General Hospital, Patient Explanation: Prostate Rebore Surgery (TURP). South Australia2) Addenbrooke’s Hospital, Cambridge University Hospital NHS Foundation Trust, Patient Information Department of Urology: Transurethral resection of the prostate: procedure-specific information.3) Queensland Government, Transuretheral Prostatectomy (TURP) & open.4) Dept of Health, Government of WA, Consent form for transurethral resection of prostate (TURP).5) BAUS consent form for transurethral incision or resection of prostate.






