Download

1 / 32
320 likes | 513 Vues
Population Surveys Scopes , Prevalence , Incidence , Health Registries. Ettore Beghi Institute for Pharmacological Research Mario Negri, Milano, Italy. SCOPE OF POPULATION SURVEYS. Measure prevalence Measure incidence Measure mortality Identify cases for case-control studies

E N D
PopulationSurveysScopes, Prevalence, Incidence, HealthRegistries Ettore Beghi InstituteforPharmacologicalResearch Mario Negri, Milano, Italy
SCOPE OF POPULATION SURVEYS • Measure prevalence • Measure incidence • Measure mortality • Identify cases for case-control studies • Identify exposures for cohort studies • Study familial aggregation/genetics • Screen candidates for prevention/early treatment
ANATOMY OF A POPULATION SURVEY • Definitionof the studypopulation • Definitionofdisease • Case ascertainment (prevalence, incidence and mortality) • Calculationofepidemiologicalindexes • Distributionbytime, place & person
DIAGRAM OF THE IDENTIFICATION OF A DISEASE IN THE GENERAL POPULATION Kurtzke, 1978
HOW TO DEFINE A POPULATION • Geographicboundaries - Residency - Istituzionalization - Migration • Temporalboundaries - Prevalenceperiod (point, period, lifetime) - Incidenceperiod
MEASURES OF DISEASE FREQUENCY • INCIDENCE: Number of individuals in a population that become ill in a stated period of time • CUMULATIVE INCIDENCE: Proportion of a fixed population that becomes ill in a stated period of time • PREVALENCE: Proportion of a population affected by a disease at a given point of time • MORTALITY: Number of individuals in a population died for a disease in a stated period of time
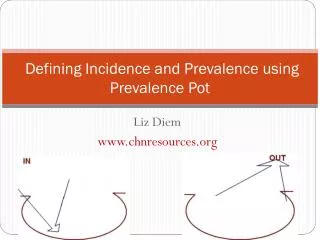
PREVALENCE AND INCIDENCE Prevalence = Incidence x average duration Incidence Migrating in Migrating out Prevalence Death Recovery
SOURCES OF NEUROLOGICAL DISEASES IN EPIDEMIOLOGICAL STUDIES • Hospital records • Ambulatoryrecords • Electrophysiological (EMG) records • Generalpractitioners’ files • Disabilityrecords • Layassociations • Tertiarycenters • Death certificates • Diagnosisrelatedgroups (DRGs) • Diseaseregistries
MIGRAINE IS A HETEROGENEOUS AND ILL-DEFINED CLINICAL CONDITION • Intensity, duration, frequency and characteristics of attacks tend to vary in the general population • In each patient, symptoms may vary with time • Many individuals may have different types of headache • Many individuals do not consult their doctor for headache
MIGRAINE WITHOUT AURA (IHS, 1988) • A. At least 5 attackswithcriteria B-D • B. Attackslasting 4-72 hr (no or poor treatment) • C. Headachewith at leasttwofeatures: - Unilateral - Pulsating - Moderate or severe • D. At leastoneamong: - Nausea and/or vomiting - Photophobia and/or phonophobia • E. At leastoneof the following: - Otherdisturbancesexcludedbyhx and examination - Otherdisturbancesexcludedbydiagnostictests - Otherdisturbances, butmigraineattacksverified
CHANGE IN THE PREVALENCE OF MIGRAINE WHEN VARYING THE NUMBER OF IHS DIAGNOSTIC CRITERIA Merikangaset al, 1990
EPILEPSY AND EPILEPTIC SEIZURES • EPILEPSY= Clinicalconditioncharacterizedbyrepeatedunprovokedseizures • UNPROVOKED SEIZURE= Seizureoccurring in the absenceofknownprecipitants; itmayoccur at the presenceof a non-recent CNS injury • ACUTE SYMPTOMATIC SEIZURE = Seizureoccurring in closetemporalrelationshipwithan acute CNS insult
EPILEPSY, ACTIVE & IN REMISSIONDefinitions • ACTIVE EPILEPSY:epilepsy currently being treated or whose most recent seizure has occurred (usually) within the past two to five years (Thurman et al, Epilepsia, 2011) • EPILEPSY IN TERMINAL REMISSION: absenceofseizuresfor 2 or 5 yearswithoutAEDs
ACUTE SYMPTOMATIC SEIZURESInterval from precipitating factor Epidemiology Task Force, Epilepsia 2009
EPIDEMIOLOGICAL INDEXES OF EPILEPSY IN INDUSTRIALIZED COUNTRIES • IncidenceEpilepsy 29-53 100,000/yrEpilepsy+singleseizures 73-86 Acute symptseizures 20-30 Status epilepticus 10-40 • Cumulative incidence 1-3% • PrevalenceActiveepilepsy 5-8 x1,000 Lifetime 15-50 • Mortality 1-4 x100,000/yr • SMR 2-3
DeCarli, LancetNeurol 2003: 2:15
PREVALENCE OF COGNITIVE IMPAIRMENT ACCORDING TO CLINICAL DEFINITION DeCarli, LancetNeurol 2003: 2:15
PROBLEMS REGARDING THE DIAGNOSIS OF POLYNEUROPATHY • The majority of the available data comes from clinical series • The diagnosis of polyneuropathy is based on clinical and elettrophysiological features • Polyneuropathy includes a wide spectrum of disorders ranging from symptomatic clinical conditions to subclinical variants • Diagnosis should be confirmed by a neurologist
Polyneuropathy in the ElderlyPrincipalSymptoms • Muscle cramps • Restless legs syndrome • Burning feet • Muscle pain • Problems with handling objects • Impairment of standing and gait • ‘Glove’ and ‘stocking’ paresthesiae
POLYNEUROPATHY IN THE ELDERLYValidityof the screening questions Monticelli et al, Neuroepidemiology 1993
POLYNEUROPATHY IN THE ELDERLYInter-rater agreement (kappa statistic) Monticelli et al, Neuroepidemiology 1993
EL ESCORIAL CRITERIA FOR THE DIAGNOSIS OF ALS • Based on the topographical location of upper (UMN) and lower motor neuron (LMN) signs in 4 CNS regions, progression of these signs, and absence of other diseases • Degree of diagnostic certainty (definite, probable, possible, suspected ALS) based on a different combination of UMN and LMN signs Brooks, 1994
EL ESCORIAL CRITERIA FOR THE DIAGNOSIS OF ALS • DEFINITE ALS - LMN and UMN signs in 3 spinal regions - LMN and UMN signs in the bulbar region and in 2 spinal regions • PROBABLE ALS - LMN and UMN signs in 2 spinal regions • POSSIBLE ALS - LMN and UMN signs in 1 region - UMN signs in 2 or more regions - LMN signs rostral to UMN signs • SUSPECTED ALS - LMN signs in 2 or more regions Source: J Neurol Sci 1994; 124 (suppl): 96-107
DISEASE REGISTRIES • Lists of diseases (or disease groups) in well-defined populations • Collection of data on disease burden and identification of patients’ cohorts to be followed for specific purposes • For rare diseases, registries represent a (re)source for the collection of sizable numbers of cases for focused studies
EXPLANATIONS FOR HIGHER AND MORE HOMOGENEOUS RATES IN EUROPEAN REGISTRIES • Prospective inception of cases • Multiple sources • Fairly complete case ascertainment • Continuous surveillance • Use of the same diagnostic criteria
OBJECTIVES OF A POPULATION-BASED REGISTRY • Incidence and prevalence of the target condition • Temporal and geographic trends of the disease • Full clinical spectrum of the disease • Clinical and paraclinical markers of the disease • Practical management and socio-economic implications of the disease • Data banks for clinical/biological material
PREREQUISITES FOR THE START OF A REGISTRY • Definition of the population at risk • Selection of the best source(s) of cases • Choice of the correct diagnostic criteria
SOURCES OF CASES • Hospital records • Outpatient records • Neurophysiology units’ archives • General practitioners’ files • Disability records • Lay associations’ files • ALS centers • Death certificates • Administrative files (hospital discharge diagnoses)
THE EURALS CONSORTIUM • Ireland 5.0M • Scotland 5.0M • Lancashire & Cumbria 1.8M • London 2.8M • Italy (all) 8.0M • Belgrade 2.0M • Madrid 1.0M • Limousin 0.7M • Germany ? • Russia ? • Israel ? • Total >25M
PRACTICAL RECOMMENDATIONS TO START A POPULATION-BASED REGISTRY • Select a well-defined geographic area • Identify one or more accessible sources • Use valid and reliable diagnostic criteria • Set a network of specialists able to trace all cases residing in the area • Select a number of core variables to verify the correctness of the diagnosis and define the general profile of the disease • Start specific studies only after preparing ad-hoc protocols and case collection forms