Download
1 / 1

E N D
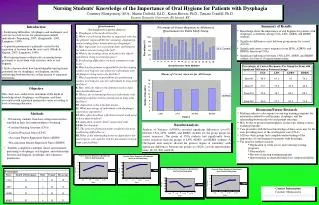
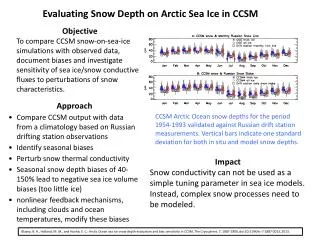
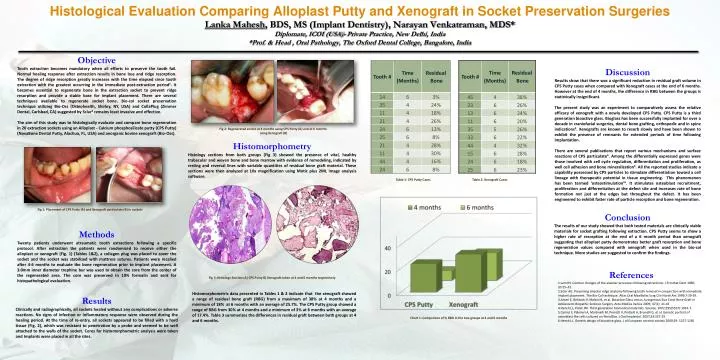
Histological Evaluation Comparing Alloplast Putty and Xenograft in Socket Preservation SurgeriesLanka Mahesh, BDS, MS (Implant Dentistry), Narayan Venkatraman, MDS*Diplomate, ICOI (USA)- Private Practice, New Delhi, India*Prof. & Head , Oral Pathology, The Oxford Dental College, Bangalore, India Objective Tooth extraction becomes mandatory when all efforts to preserve the tooth fail. Normal healing response after extraction results in bone loss and ridge resorption. The degree of ridge resorption greatly increases with the time elapsed since tooth extraction with the greatest occurring in the immediate post-extraction period1. It becomes essential to regenerate bone in the extraction socket to prevent ridge resorption and provide a stable base for implant placement. There are several techniques available to regenerate socket bone. Bio-col socket preservation technique utilizing Bio-Oss (Osteohealth, Shirley, NY, USA) and CollaPlug (Zimmer Dental, Carlsbad, CA) suggested by Sclar2 remains least invasive and effective. The aim of this study was to histologically evaluate and compare bone regeneration in 20 extraction sockets using an Alloplast - Calcium phosphosilicate putty (CPS Putty) (NovaBone Dental Putty, Alachua, FL, USA) and anorganic bovine xenograft (Bio-Oss). Discussion Results show that there was a significant reduction in residual graft volume in CPS Putty cases when compared with Xenograft cases at the end of 6 months. However at the end of 4 months, the difference in RBG between the groups is statistically insignificant. The present study was an experiment to comparatively assess the relative efficacy of xenograft with a newly developed CPS Putty. CPS Putty is a third generation bioactive glass. Bioglass has been successfully implanted for over a decade in craniofacial surgeries, dental bone grafting, orthopedic and in spine indications3. Xenografts are known to resorb slowly and have been shown to exhibit the presence of remnants for extended periods of time following implantation. There are several publications that report various mechanisms and surface reactions of CPS particulate4. Among the differentially expressed genes were those involved with cell cycle regulation, differentiation and proliferation, as well cell adhesion and bone mineralization5. All the reported studies indicate a capability possessed by CPS particles to stimulate differentiation toward a cell lineage with therapeutic potential in tissue engineering. This phenomenon has been termed ‘osteostimulation’6. It stimulates osteoblast recruitment, proliferation and differentiation at the defect site and increases rate of bone formation not just at the edges but throughout the defect. It has been engineered to exhibit faster rate of particle resorption and bone regeneration. Fig 2: Regenerated socket at 4 months using CPS Putty (A) and at 6 months using Xenograft (B) Histomorphometry Histology sections from both groups (Fig 3) showed the presence of vital, healthy trabecular and woven bone and bone marrow with evidence of remodeling, indicated by resting and reversal lines with variable quantities of residual bone graft material. These sections were then analyzed at 10x magnification using Motic plus 2ML image analysis software. Table 1: CPS Putty Cases Table 2: Xenograft Cases Fig 1: Placement of CPS Putty (A) and Xenograft particulate (B) in sockets Conclusion The results of our study showed that both tested materials are clinically viable materials for socket grafting following extraction. CPS Putty seems to show a higher rate of resorption at the end of a 6 month period than xenograft suggesting that alloplast putty demonstrates better graft resorption and bone regeneration values compared with xenograft when used in the bio-col technique. More studies are suggested to confirm the findings. Methods Twenty patients underwent atraumatic tooth extractions following a specific protocol. After extraction the patients were randomized to receive either the alloplast or xenograft (Fig. 1) (Tables 1&2), a collagen plug was placed to cover the socket and the socket was stabilized with mattress sutures. Patients were recalled after 4-6 months to evaluate the bone regeneration prior to implant placement. A 3.0mm inner diameter trephine bur was used to obtain the core from the center of the regenerated area. The core was preserved in 10% formalin and sent for histopathological evaluation. • References • Lam RV. Contour changes of the alveolar processes following extractions. J Prosthet Dent 1960; 10:25–32. • Sclar AG. Preserving alveolar ridge anatomy following tooth removal in conjunction with immediate implant placement. The Bio-Col technique. Atlas Oral Maxillofac Surg Clin North Am.1999;7:39-59. • Ameri E, Behtash H, Mobini B, et al. Bioactive Glass versus Autogenous Iliac Crest Bone Graft in Adolescent Idiopathic Scoliosis Surgery. Acta Medica Iranica 2009; 47(1): 41-45 • Hench LL, Polak JM. Third-generation biomedical materials. Science. 2002;295(5557):1014-7. • Carinci F, Palmieri A, Martinelli M, Perrotti V, Piattelli A, Brunelli G, et al. Genetic portrait of osteoblast-like cells cultured on PerioGlas. J Oral Implantol. 2007;33:327-33 • Hench LL. Genetic design of bioactive glass. J of European ceramic society 2009;29: 1257-1265 Fig 3: Histology Sections A) CPS Putty B) Xenograft taken at 4 and 6 months respectively Histomorphometric data presented in Tables 1 & 2 indicate that the xenograft showed a range of residual bone graft (RBG) from a maximum of 38% at 4 months and a minimum of 18% at 6 months with an average of 25.7%. The CPS Putty group showed a range of RBG from 30% at 4 months and a minimum of 3% at 6 months with an average of 17.4%. Table 3 summarizes the differences in residual graft between both groups at 4 and 6 months. Results Clinically and radiographically, all sockets healed without any complications or adverse reactions. No signs of infection or inflammatory response were observed during the healing period. At the time of re-entry, all sockets appeared to be filled with a hard tissue (Fig. 2), which was resistant to penetration by a probe and seemed to be well attached to the walls of the socket. Cores for histomorphometric analysis were taken and Implants were placed in all the sites. Chart 1: Comparison of % RBG in the two groups at 4 and 6 months