Download
1 / 29
310 likes | 849 Vues
An Evaluation of the use of reformatted coronal oblique proton density fat suppressed fast spin echo images in ACL tears. Joseph Castillo B.Sc M.Sc. Introduction. MR evaluation of the ACL is not done in isolation but is part of a routine knee protocol.

E N D
An Evaluation of the use of reformatted coronal oblique proton density fat suppressed fast spin echo images in ACL tears Joseph Castillo B.Sc M.Sc
Introduction • MR evaluation of the ACL is not done in isolation but is part of a routine knee protocol. • MR diagnoses of the ACL are usually based on oblique sagittal and coronal images using T1, T2, GRE and STIR sequences.
Limitations • The unique diagonal course and its size of 3.5cm pose limitations to standard imaging. • Partial volume effects of the ACL with adjacent soft tissues is the commonest limitation • Another limitation with sagittal view is the pulsating artifact from the popliteal artery.
Strategies • Knee flexion. • Oblique sagittal images prescribed parallel to lateral femoral condyle using an axial image. • Oblique sagittal images prescribed parallel to ACL using a coronal image • Use of 3D GRE. • Supplementing with axial imaging. • Use of secondary signs.
Thin slice direct coronal obliques • Two studies used thin slice direct coronal obliques prescribed parallel to ACL using a sagittal image. (Katahira et al, 2001 and Hong et al 2003) • Increased Diagnostic Accuracy • Increased Diagnostic Efficacy • Increased Scanning time by 4min.
Grading the Severity of ACL injury • Grading of the ACL injury on MRI can be of help during the treatment decision making process. Not every one who has an ACL partial tear requires ACL injury requires surgical reconstruction. In this regard it would be beneficial to be able to determine whether the ACL injury is classified as low or high grade partial tear.
Purpose of the Study • indirect coronal oblique image batch reformatted from an optimized coronal high resolution (2mm) slices along the course of the ACL would provide additional information on the status of the anterior cruciate ligament without prolonging scanning time.
Scanning Parameters • TR 4200ms • TE 20 • ETL 3 (Kojima et al, 1999) • RBW 20.83 • Matrix 256 x 256 • FOV 24 • Slice 2mm gap 0 • Fat suppression
Equipment • 1.5T whole-body scanner (GE Medical Systems, Milwauke, Wisconsin) operating with Twin Speed gradients. • A dedicated transmit-receive coil. • Patient positioned with knee slightly flexed and with a slight external rotation.
Materials and Methods • Patients could be of either gender. • Had a history of trauma • Had a request to assess ACL and/or menisci pathology by MRI • had never undergone ACL repair • This criteria yielded 87 patients. • A review of MRI reports disclosed 10 partial tears.
Results • Images were reviewed by 2 radiologists independently • Initially, each radiologist evaluated the status of ACL by routine knee protocol (A) • A – Coronal PD, Sagittal PD, Coronal STIR, Sagittal T2*
Results • Then later (after 10days) in combination with reformatted coronal oblique images (Protocol B) • And later on (10days), using the reformatted coronal oblique images on their own (Protocol C)
Diagnostic Accuracy • Interreader agreement for the presence or absence of ACL Tear was measured using Confidence levels (5 point scale): • 0 – intact, 1 – probably intact, 2 – possible tear, 3 – probably tear, 4 – definite tear
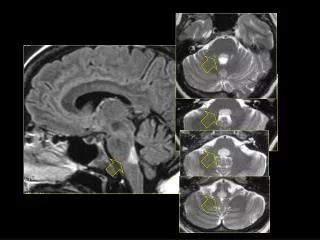
MR Grading Criteria – Grade 0 • Intact ligament. A and B, sagittal PD-fs (TR/TE 4200/20) show normal ACL and sagittal T2* (TR/TE/FA 600/15/20) show almost normal ACL but with some high signal at the tibial attachment. C. RCO shows normal contour with distinct fibers at the tibial attachment
Grade 1 – low grade partial tear • A, sagittal PD-fs and B, sagittal T2* shows more than half of the ligament substance disrupted at the midportion and tibial attachment of the ACL which suggests a high grade tear. C, RCO shows oedematous ACL with diffusely increased signal intensity, but ligament continuity at both femoral and tibial sites are preserved. Low grade partial tear is more likely.
Grade 2 – High Grade partial tear • A, Sag PD-fs and B Sag T2* show ACL disruption at the Femoral attachment. C, RCO shows marked thinning (more than half of the ACL disrupted) but with preserved continuity. High grade partial tear was suggested by both readers.
Grade 3 – Complete tear • A PD-fs, B T2* GRE and C (RCO) show a complete tear of the ACL.
Results • Interreader agreement was calculated using weighted statistics. • 0.0 < < 0.2 Poor correlation • 0.2 < < 0.4 Fair correlation • 0.4 < < 0.6 Moderate correlation • 0.6 < < 0.8 Good correlation • 0.8 < < 1.0 Very Good correlation
Confidence – Protocol A • Interreader agreement for the presence or absence of ACL tear
Confidence – Protocol B • Interreader agreement for the presence or absence of ACL tear
Confidence – Protocol C • Interreader agreement for the presence or absence of ACL tear
Confidence – all protocols • Protocol A – Moderate correlation • Protocol B – Good correlation • Protocol C – Poor correlation
Grading – Protocol A • Interreader agreement for grading the ACL without the reformatted coronal oblique images.
Grading Protocol B • Interreader for grading ACL using protocol A and the indirect coronal oblique
Grading Protocol C • Interreader agreement using the reformatted coronal obliques only
Limitations of the study • Indirect signs were not removed • Due to small number of cases this study was exploratory. • Radiologists viewed printed images rather than using the advantage windows system. • A comparison of sensitivity and specificity using arthroscopic findings could have added value to the study.
Conclusion • I found that the use of additional reformatted coronal oblique images improved the accuracy of ACL tear detection. • Reformatted oblique coronal images also improved the accuracy of grading ACL injury and can help in the decision making process for treatment.