Download
1 / 12
130 likes | 286 Vues
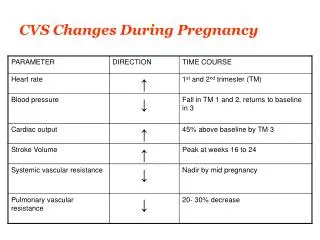
Torsional Changes During Routine Ophthalmic Anesthesia. The authors have no financial interest in the subject matter of this e -poster. . Eunice Yook , BS, MS, John P. Hatch, PhD, Kent L. Anderson, MD, PhD Department of Ophthalmology

E N D
Torsional Changes During Routine Ophthalmic Anesthesia The authors have no financial interest in the subject matter of this e-poster. Eunice Yook, BS, MS, John P. Hatch, PhD, Kent L. Anderson, MD, PhD Department of Ophthalmology The University of Texas Health Science Center at San Antonio,
ABSTRACT Purpose: The purpose of this study is to investigate the torsional changes of the eye after anesthesia during cataract extraction. With this information, we hope to augment current practices by determining whether pre-anesthesia markings are indicated before cataract surgery, especially when using toric lenses. Methods: This study recruited 30 patients from a clinic affiliated with a medical university in San Antonio, Texas. Before anesthesia was administered, the medial and lateral canthus was marked with a sterile marking pen in the upright position. Next, using a Bubble Level Toric Marking System, marks were made at the medial and lateral limbus. A photo was obtained at a fixed distance. After anesthesia was administered, a second photo was taken. Differences were measured using a screen protractor, and results were analyzed in IBM SPSS for Windows. Results: Pre-anesthesia and post-anesthesia photos were taken and compared in 30 eyes. Mean cyclotorsion was 4.20° with a standard deviation of 3.05°. Values ranged from 0.18° to 10.02°.The 95% confidence interval was 3.06-5.33°. Conclusion: Previous studies have found clinically significant alterations of postoperative refractions at 15°. Our study showed all subjects had less than a 15° change, suggesting that pre-anesthesia markings may not be required. Instead, the surgeon can mark the eye intraoperatively after anesthesia has been administered to guide placement of toric lenses.
INTRODUCTION • Several factors may affect ocular torsion: • Changes in position (supine vs. upright) • Extra-ocular muscle paralysis • Rotation of the intraocular lens (IOL) in the bag • In regards to positional influences, the current agreement is that regardless of correcting for position, postoperative results are the same1.
INTRODUCTION • Since extra-ocular muscles contribute to the tone, curve and position of the eyeball when contracted1 (Figure 1), anesthesia induced muscle paralysis may affect eye position during ocular surgery2. • Torsional effects during anesthesia are currently unknown.
INTRODUCTION • Astigmatism • Torsional changes will affect those with astigmatism. • New toric IOLS can correct for astigmatism, but require • precise positioning, and are not covered by insurance. • Previous studies have shown that a change more than 15° • in the axis during refractive surgery reduces the amount of • astigmatism corrected by 50%4,5. • If anesthesia causes a significant cyclotorsion, surgeons may • find it beneficial to mark the eye before anesthesia. • Therefore, by investigating torsional changes under • anesthesia, one can determine whether preoperative • markings are indicated for cataract surgery.
STUDY DESIGN • Prospective • Noncomparative • Enrollment of 30 patients • Subjects recruited from a clinic affiliated with a large medical university in San Antonio, Texas. Inclusion criteria • Patients who were cleared exclusively for routine cataract extraction with IOL placement.
METHODS Pre-anesthesia: • Eyelid marked in the upright position. • Temporal and nasal limbus marked with Mastel Bubble Level Toric Marking System. (Figure 2) • Sony Cybershot Camera in Easy Mode camera was used to obtain a photo of the eye at a fixed distance. (Figure 3a, 4a) Figure 2: Mastel Bubble Level Toric Marking System Figures 3a and 3b: Position of surgical eye pre-local anesthesia and post-local anesthesia, respectively. a. Pre-anesthesia: b. Post-anesthesia:
METHODS Post-anesthesia: • Second photo was taken after the presence of extra-ocular muscle paralysis (Figure 3b, 4b). • Effect of anesthesia was confirmed by presence of chemosis, a reaction to the anesthesia. (Figure 3b). • Differences measured using the Iconico Screen Protractor. • Results were analyzed in Excel.
METHODS Figures 3a and 3b: Position of eye pre- and post retrobulbar anesthesia, respectively. Figures 4a and 4b: Position of eye pre- and post local anesthesia, respectively. a. Pre-anesthesia: a. Pre-anesthesia: b. Post-anesthesia: b. Post-anesthesia: Area of conjunctivalchemosis Figures 3a and 3b: Position of surgical eye pre-local anesthesia and post-local anesthesia, respectively. a. Pre-anesthesia: b. Post-anesthesia: Figures 2a and 2b: Position of surgical eye pre-retrobulbar anesthesia and post–retrobulbar anesthesia, respectively. Figures 2a and 2b: Position of surgical eye pre-retrobulbar anesthesia and post–retrobulbar anesthesia, respectively. a. Pre-anesthesia: a. Pre-anesthesia: b. Post-anesthesia: b. Post-anesthesia: Area of conjunctival chemosis Area of conjunctival chemosis
RESULTS • Pre-anesthesia and post-anesthesia photos were taken and compared in 30 eyes. • After statistical analysis, mean cyclotorsion was 4.20° with a standard deviation of 3.05°. • The change in torsion varied from 0.18° to 10.02°. • The 95% confidence interval was 3.06-5.33°. • Data was tested with a one-sided single sample t-test at a 0.05 level of significance, using IBM SPSS for Windows (IBM SPSS, Chicago, Ill.),
CONCLUSIONS • After studying 30 subjects, we found that the anesthesia • effects did not move the eye greater than 15°. • Clinical significance • Previous studies found clinically significant effects on • postoperative refraction at 15°4,5. • Our study showed subjects had less than a 15° change, • therefore pre-anesthesia markings may not be necessary. • Instead, the surgeon can mark the eye after anesthesia • has been administered to guide IOL placement. • When combined with other factors that affect • torsion, the additive effects may exceed 15° leading to • poor refraction outcomes.
REFERENCES Dooley I, Charalampidou S, Malik A, Ormonde G, Loughman J, Molloy L,Beatty S. Surgically induced astigmatism after phacoemulsification with and without correction for posture-related ocular cyclotorsion. J Cataract Refract Surg. 2010; 36: 413-7. Kraft SP, O'Reilly C, Quigley PL, Allan K, Eustis HS. Cyclotorsion in unilateral and bilateral superior oblique paresis.JPediatrOphthalmol Strabismus. 1993 Nov-Dec;30(6):361-7. Lynch PJ, illustrator; Jaffe CC. Yale University Center for Advanced Instructional Media Center for Advanced Instructional Media, 1987-2000. Accessed on September 8, 2010 at http://commons. wikimedia.org/wiki/File:Eye_movements_abductors.jpg. Novis C, Astigmatism and Toric Lenses. Current Opinion in Ophthalmology. 2000, 11:47–50. Tjon-Fo-Sang, MJ, de Faber JH, Kingma C, Beekhuis WH. Cyclotorsion: A possible cause of residual astigmatism in refractive surgery. J Cataract Refract Surg. 28; 4:599 – 602. Figures 3a and 3b: Position of surgical eye pre-local anesthesia and post-local anesthesia, respectively. a. Pre-anesthesia: b. Post-anesthesia: Figures 2a and 2b: Position of surgical eye pre-retrobulbar anesthesia and post–retrobulbar anesthesia, respectively. Figures 2a and 2b: Position of surgical eye pre-retrobulbar anesthesia and post–retrobulbar anesthesia, respectively. a. Pre-anesthesia: a. Pre-anesthesia: b. Post-anesthesia: b. Post-anesthesia: Area of conjunctival chemosis Area of conjunctival chemosis