Download
1 / 17
170 likes | 349 Vues
Female Reproductive System Anatomy-Histology Correlate. By: Michael Lu, Class of ‘07. Note the sacrotuberal and sacrospinous ligaments forming the greater and lesser sciatic foramens with the pelvis bones.

E N D
Female Reproductive SystemAnatomy-Histology Correlate By: Michael Lu, Class of ‘07
Note the sacrotuberal and sacrospinous ligaments forming the greater and lesser sciatic foramens with the pelvis bones. • Note the piriformis muscle posteriorly and the obturator internus muscle laterally. The specialization of the obturator fascia, called the tendinous arch, provides attachment for the levator ani muscles of the pelvic diaphragm. • The pelvic diaphragm consists of the coccygeus, puborectalis, pubococcygeus, and iliococcygeus muscles. The last 3 muscles form the levator ani muscle. • Note the relative locations of the urethra, vagina, and rectum.
NOTE: • The ovarian arteries branch off the abdominal aorta near the kidneys. The right ovarian vein drains directly into the inferior vena cava, while the left ovarian vein drains into the left renal vein and then into the inferior vena cava. Note how the vessels cross over the ureters and enter and exit the inguinal canal with the spermatic cord via the deep and superficial inguinal rings, respectively. • The arterial supply of the pelvis is supplied by the common iliac arteries, which are the end branches of the abdominal aorta. The common iliac arteries branch into the external iliac arteries (which continue as femoral arteries) and the internal iliac arteries. • The posterior division of the internal iliac artery gives off the iliolumbar, lateral sacral, and superior gluteal arteries. • The anterior division gives off the umbilical artery, which further branches off as the superior vesical artery and the medial umbilical ligament (obliterated umbilical artery. The anterior division also gives off the obturator, uterine, vaginal, middle rectal, inferior gluteal, inferior vesical, and internal pudendal arteries.
NOTE: • - The sacral plexus includes contributions from L4 to S4. The lumbosacral trunk combines L4 and L5. Note the superior gluteal artery between L5 and S1. • sciatic nerve: two separate nerves that are usually fused together – tibial nerve from L4 to S3 and common fibular nerve from L4 to S2; runs under the piriformis muscle through the greater sciatic foramen. • superior gluteal nerve: from L4 to S1; runs over the piriformis muscle through the greater sciatic foramen. • inferior gluteal nerve: from L5 to S2; runs inferior to the piriformis muscle through the greater sciatic foramen. • nerve to quadratus femoris muscle: from L4 to S1; inferior to the piriformis muscle through the greater sciatic foramen. • nerve to obturator internus muscle: from L5 to S2; exits under the piriformis muscle through the greater sciatic foramen, reenters through the lesser sciatic foramen. • posterior femoral cutaneous nerve: from S1 to S3; inferior to the piriformis muscle through the greater sciatic foramen. • pudendal nerve: from S2 to S4; exits under the piriformis muscle through the greater sciatic foramen, reenters through the lesser sciatic foramen into the pudendal canal.
The internal pudendal artery enters the perineum from the pudendal canal and gives off the inferior rectal artery. As the internal pudendal artery continues toward the external genitalia, it gives off the perineal artery superior to the perineal membrane and ends as the posterior labial artery. The internal pudendal artery continues deep to the perineal membrane, with its terminal branches ending as the dorsal artery and deep artery of the clitoris. • The pudendal nerve gives off the inferior rectal nerve, and continues as the perineal nerve superiorly and ends as the posterior labial nerve. The deep branch of the pudendal nerve continues as the dorsal nerve of the clitoris in the deep perineal space. • Reminder: The internal pudendal vessels and pudendal nerve exit the greater sciatic foramen and reenter the pelvis through the lesser sciatic foramen. From there they enter the pudendal canal and exit into the perineum.
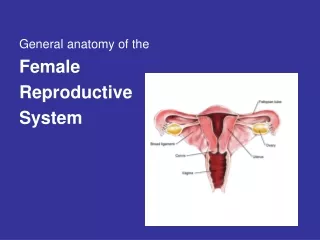
Note the relative relations of the pelvic viscera: urinary bladder, uterus, fallopian tubes, ovaries, and rectum. • Note the round ligament of the uterus connecting the lateral surface of the uterus to the inner aspect of the labium majus via the superificial inguinal ring, inguinal canal, and deep inguinal ring. It is the remnant of the gubernaculum that holds the fundus of the uterus forward. • Note the peritoneal fold reflecting from the rectum to the posterior fornix of the vagina called the rectouterine pouch, and from the uterus onto the posterior margin of the superior surface of the uterus called the vesicouterine pouch. • As the peritoneal layers hang over the uterine or fallopian tubes, they “double up” to form the broad ligament, which consists of the mesosalpinx (associated with the fallopian tubes), mesovarium (associated with the ovaries), and mesometrium (associated with the uterus). Note also the ovarian ligament between the ovary and uterus and the suspensory ligament that contains the ovarian vessels.
The list above has superficial features of the female external genitalia. • Note the fallopian tubes: fimbriae, infundibulum, ampulla, isthmus, and uterine parts. Note the various parts of the uterus, cervix, and vagina as well. • Histological slides are shown next.
The uterine or fallopian tubes, or oviduct, contain complex mucosal folds with distinct ciliated columnar epithelium. The ampulla (top left) shows the oviduct in low power. In the inset, small arrows point to ciliated cells, while arrowheads point to bulging, non-ciliated secretory (peg) cells. • The funnel-shaped opening called the infundibulum contains many finger-like projections called fimbriae (bottom left). During ovulation, the fimbriae get close to the ovary and help to sweep the ovum that is released into the abdominal cavity. • As the oviduct approaches the uterus, the mucosal folds become less complex. The uterine or interstitial portion (bottom right) contains a relatively simple lumen and columnar epithelium.
The uterus is divided into endometrial (E), myometrial (M), and perimetrial (P) layers (top left). The endometrium prepares for implantation of an ovum by cycling through proliferative and secretory phases. It can be divided into the basal and functional layers. The basal layer remains relatively unchanged through the cycles. • The proliferative phase (bottom left) is characterized by long, relatively straight endometrial glands, as indicated by the arrows. • Immediately following ovulation, the glandular epithelial cells, many of which may be ciliated, exhibit “basal vacuolization” (bottom right), which is the accumulation of glycogen in the basal cytoplasm.
The most characteristic change in the secretory phase of the endometrium is the “saw-tooth” or “serrated” appearance of the glands (top left). • The serrated endometrial glands are magnified in the bottom right panel. Note the abundance of coiled or spiral arteries that supply the entire functional endometrium. The secretory cells are also shorter with rounder nuclei than those during the proliferative phase. • During menstruation, the endometrial surface epithelium undergoes ischemia, which weakens the vascular walls resulting in hemorrhage (bottom right). The endometrial surface lacks epithelium, the uterine glands open onto the surface (large arrow), and there may be some blood clots (small arrows).
The cervix is shown in three different magnifications in the top panel. The red arrows point to the junction and change in epithelium, from the columnar epithelium of the cervical canal to the stratified, squamous epithelium of the vagina. • This is known as the strato-columnar junction, and earliest signs indicative of cervical cancer occur at this junction. • The cervical canal contains complex folds that resemble glands. The epithelium contains simple, tall columnar mucus-secreting epithelial cells. • The cervix also contains much smooth muscle and dense connective tissue.
The vagina wall contains abundant connective tissue with large amounts of elastin. There is also a thick muscular layer (bracket in top panel). The inset shows the muscular layer in more detail, with longitudinal and circular smooth muscle layers. • The adventitia contains large nerves and arteries that blend with the connective tissue of the pelvis. • The vaginal epithelium (bottom panel) is covered with non-keratinized stratified squamous epithelium that contain abundant glycogen in the cytoplasm. The glycogen is released into the vaginal lumen, where bacterial action produces lactic acid to acidify the mucosa and protect it. • The arrows indicate surface cells that can be collected for Pap smears to provide information on hormonal status and any abnormalities.
Note the normal position of the uterus. • The term “-version” refers to the angle between the long axis of the uterus and the long axis of the vagina. • The term “-flexion” refers to the long axis of the uterine body compared to the long axis of the uterine cervix. • Shown on the left are the various positions of the uterus within the pelvis. • In the following slides, we will conclude by looking at the ovary and going through the various stages of the development of the ovum and follicle. • Shown to the right is a schematic of the oval cycle. Unlike the male testis, the female ovary already contains all of its oocytes at birth. • Primordial follicles develop into primary follicles, followed by mature Graafian follicles. When the follicle ruptures, it releases the ovum to travel through the fallopian tubes to the uterus. The follicle continues to develop into the corpus luteum and corpus albicans.
The hilus of the ovary is where all the nerves and vessels enter the organ. The medulla contains loose connective tissue, abundant blood vessels and lymphatics, and nerves. The numbers in the top left panel indicate the stages of follicular development. • The surface epithelium of the ovary (bottom left) is called the mesothelium, which sits on the tunica albuginea. Note the appearance of primordial follicles within the outer cortex. • The oocyte continues to grow at the same time follicular or granulosa epithelial cells continue to divide and form multiple layers (multilaminar), as shown in the bottom right).
The top panel shows a primary follicle. The multilayered granulosa cells secrete a glycoprotein and proteoglycan rich fluid that accumulates in the spaces between the cells. • Note how the granulosa cells are separated by the surrounding stromal or thecae by a distinct basement membrane (arrows). • The oocyte is surrounded by a prominent glycoprotein coat called the zona pellucida (ZP). • With further development, there is a single fluid-filled space called an antrum. This is characteristic of a secondary follicle (bottom panel). • The oocyte is supported by a mound of granulosa cells called the cumulus oophorus. The oocyte is still surrounded by the zona pellucida, and outside the zona pellucida are some granulosa cells that may accompany the oocyte when it is ovulated. This layer of granulosa cells outside the zona pellucida is known as the corona radiata. • The thecal cells also continue to differentiate into theca interna and externa cells with specialized functions, as shown in the next slide.
The stromal theca interna cells (top left) lie immediately outside the granulosa cells, separated by the basement membrane. The theca interna cells are larger and paler staining than regular stromal cells or the surrounding theca externa cells. The interna cells produce steroid precursors that are converted to estrogen by the granulosa cells. • If the ovum is fertilized and implanted in the uterus, the mature follicle converts into the corpus luteum (bottom left; CL), or yellow body. It acts as an endocrine organ that secretes progesterone. Note the formation of inner granulosa lutein and outer theca lutein cells. • The bottom right panel compares the granulosa lutein cells (GLC) with the theca lutein cells (TLC).
If the ovum is not fertilized, it is expelled from the uterus with menstruation. The corpus luteum degenerates and forms the corpus albicans (top panel), or white body. There are dense accumulations of collagen, which looks like a scar. • The corpus albicans is also formed during the later half of pregnancy after the placenta takes over the role of steroid (progesterone) secretion from the corpus luteum. • Sometimes the oocyte degenerates prior to complete maturation. It begins to shrink within the zona pellucida and most of the granulosa cells degenerate. • The follicular basement membrane thickens and becomes what is called a glassy membrane. This is the distinct identifying characteristic of an atretic follicle.