Download
1 / 33
340 likes | 710 Vues
Cognitive Behaviour Therapy (CBT) - its application to Depression & Low Self-esteem. Frank McDonald Consultation-Liaison Psychologist The Townsville Hospital for JCU Med School Year 5 Mental Health Rotation www.fmcdonald.com. Overview. What is CBT? Suitable Conditions for CBT

E N D
Cognitive Behaviour Therapy (CBT)- its application to Depression & Low Self-esteem Frank McDonald Consultation-Liaison Psychologist The Townsville Hospital for JCU Med School Year 5 Mental Health Rotation www.fmcdonald.com
Overview • What is CBT? • Suitable Conditions for CBT • Preparatory Steps • Central Concepts of Cognitive Therapy: 3 levels of thinking • Core Beliefs • Schema • Automatic Negative Thoughts (ANT’s) • ‘How to’ of Cognitive Therapy • Assessment • Managing ANT’s • Referring on option • Class Exercise: Cognitive Therapy case study formulation of depression & low self-esteem • Patient & Therapist Resources
Biological Psychological Social What is CBT ? Any significant mental health problem involves on-going interactions amongst • Biological factors genes, current biological state • Psychological factors cognitions (thoughts & schemas), affect (feelings &moods), overt behaviours • Social factorsimmediate social environment & culture Mental Health
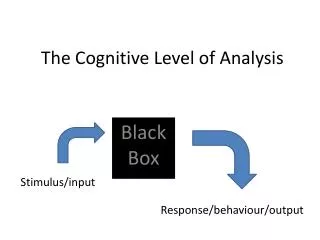
Feelings & behaviour depend on interpretation of events What is CBT ? • Cognitive Behaviour Therapy is one approach to addressing Psychological contribution to mental health issues • Based on idea that thoughts create moods, influence behaviour &alter physiological state
What is CBT ? • In CBT pt’s learn that we all have inherent tendencies to certain specific thoughts, schemas & core beliefs (more generalised ways of thinking) that can evoke unhappiness & disturbance • We can learn to spot negative thoughts as they come up & then challenge & re-think them
What is CBT ? • Cognitive Therapy usually combined with behavioural techniques or ‘experiments’ • These help pts act on their new ideas. Disconfirm their original conclusions & confirm alternative beliefs e.g. asserting self usually does not end in hostility but engenders respect • They also address behavioural excesses (e.g. avoidance) & deficits (e.g. problem-solving) • When combined, termed Cognitive Behaviour Therapy Confronting fear of heights consolidates new ideas about fear
ADHD Conduct disorder Dementia Substance abuse (including alcohol) Schizophrenia Depression Bipolar disorder Panic disorder Phobias (eg Social Phobia) Generalised anxiety disorder Obsessive-compulsive disorder Posttraumatic stress disorder Somatoform & factitious disorders Dissociative disorder Sexual disorders Eating disorders Some sleep disorders Personality disorders Marital, family and parenting problems Pain Health-related behaviours CBT empirically supported for In these diagnostic groups CBT has increasingly become the treatment of choice or a significant adjunct to pharmacological management
Preparatory steps • Is there evidence of CBT’s effectiveness with presenting problem? • Explain relationship between thinking & feeling via basic CBT model of distress e.g. Ellis’s ABC model (click link). Does pt accept it? (Many do. It’s the easiest of all psychotherapies for people to understand & apply.) • Is pt willing & able to identify & regularly work on specific problems via self-help assignments? e.g. keep written record of re-evaluations of Automatic Negative Thoughts (ANT’s)? • Willing to read suggested material (‘bibliotherapy’) to facilitate self-help?
Central concepts • Within Beck’s model of Cognitive Therapy pt interpretation of events analysed at 3 levels of thinking • 1. Core Beliefs about self, others, the world/life e.g. “I am a failure, others are always ready to attack me. The world is full of bullies, life is not fair” • Most fundamental but least conscious influence on our perceptions of events. Develop from early experience
Central concepts • Such beliefs potentially could produce state of extreme & continuous distress. But next, more intermediate level (its assumptions & rules), acts as buffer around core beliefs in engagements with self, others, & world • Unconditional & absolutist. They consist of most sensitive view of self (vulnerable, helpless, inept, loveless, worthless) & most primitive view of others (rejecting, hostile, demeaning). “I’m worthless” “I’m unlovable” “I’m a failure” “The world is hostile” “Other people hate me”
Central concepts • 2. Schemas (mental structures that organise info), assumptions &rules that allow pt to function, even if not optimally • Often expressed as conditional ‘if-then’ statements • Also may adopt rules for life - ‘shoulds’, ‘musts’ ‘oughts’ ‘needs’ - to cope • e.g. “If I show my weaknesses, thenothers will reject me. If I’m good then good things will happen. Everyone shouldapprove of me. I must try to excel, others will like me & then I don’t have to face my feelings of failure as a person. I need to have others’ approval, attention or affection (like air, water, shelter vs. prefer )”
Central concepts • 3. Automatic negative thoughts (ANT’s) or‘self-talk’ • Most accessible level of cognition • These repetitive internal words, phrases, images, meanings drive our ‘here & now’ experiences & emotional responses e.g. “I can’t face the day. Why get up? There’s nothing to live for!”
Central concepts • Initial Cognitive Therapy focus on ANT’s • Scratch the surface of almost any mood problem, like depression, & you’ll find associated self-talk e.g. “Life is such a struggle. I’ve run out of fight. I can’t face another day!” • Whether cause or effect of depressed mood, such self-talk will make depression, due to whatever cause, worse
‘How to’: Assessment • Therapy begins (& often continues) with some form of assessment to reveal presence of any of 3 cognitive factors above Can include: • Clinical interview • Self-monitoring (diaries). Central to Cognitive Therapy • Self-report questionnaires (e.g. Irrational Values Scale; John Young’s Schema Questionnaire & Client Guide) • Structured interview (e.g. Functional Analysis of who, what, when, where, thoughts & feelings, antecedents (recent & remote) & consequences, purpose served/payoffs for maintaining problem) • Observation (e.g. ‘think aloud’ technique) • Clinical records (e.g. referral notes, hospital observations)
‘How to’: Managing ANT’s • ANT’s are usually first focus of Cognitive Therapy. Become obvious from assessments & as listen to pt’s experiences & concerns • This ‘5 Steps’ handout quickly shows pts how to identify & manage ANT’s. Supplement with following handouts. Pt reading is previously agreed requirement of most Cognitive Therapy to augment therapy sessions • Cognitive_therapy_intro_for_pts Comprehensive intro to ‘cognitive restructuring’ starting with contrasting case examples • Diary Disputing pagesleads for questioning ANT’s & diary/log example • Examples_of_unhelpful_thoughts Thinking styles that cause distress • Coping_statements Shortcuts to disputation • Managing_Unhelpful_ThoughtsMore tips on self-mx of ANT’s • Disputing irrational thoughts Step by step self-mx example using Ellis’s ABC model
CBT is not teaching pts what to think or insisting logical/positive /rational/helpful thoughts always be sought out It does not usually address normal sadness or distress associated with unpleasant situations e.g. anxiety while awaiting cancer test results Rather, stages of therapy reflect objectives: i) to help pts see relationship between thinking & feeling thru identifying specific ANT’s & then ii) to help pts consider possibility of alternative ways of seeing situation. Simply inviting them. There are numerous ways to achieve this goal ‘How to’: Managing ANT’s
‘How to’: Managing ANT’s • One method: ask pt to consider questions on ‘diary disputing’ h/o (#2) in relation to a specific ANT they identify • By re-assessing, pt may recognise alternative explanations of events that may be equally valid & lead to more helpful response • More methods: See ‘Pt and Therapist Resources’ slide
‘How to’: Managing ANT’s iii) Pts then to identify changes in mood or distress levels & to record simultaneously what specific images & thoughts they were aware of & new ratings of endorsement of original beliefs after reflecting on new perspectives (see diary example below)
For many pts challenging & changing ANT’s with logic & evidence may be sufficient May well positively effect deeper levels of maladaptive thinking/assumptions (schemas & core beliefs) without direct attention to these . . . . . . or maybe not ‘How to’: Managing ANT’s
‘How to’: Referring on • If not, & distress or dysfunction remains high after working on ANT’s, further work needed e.g. on underlying Core Beliefs and/or Schema • Such fundamental ways of thinking are long-established & so usually require longer-term therapy that builds more evidence for new ways of thinking against old patterns of thought
‘How to’: Referring on • Due to time factor, GP’s usually consider referring on to Psychologists or other therapists trained in more advanced forms of CBT eg schema focussed therapy or dialectical behaviour therapy (DBT) • Also, some therapists are more familiar with attributional styles which most commonly occur in range of situations within specific disorders. They can short-cut process of identifying ANT’s & other beliefs & save therapy time See Table next slide
Class Exercise Clinically depressed 25 y.o. with low self-esteem presents for CBT after rejection by work colleague saying “I don’t know how to interact successfully with people.” “Life is such a struggle, I’ve run out of fight. I can’t face another day.” “People don’t care about me. They are trying to destroy me. I’ll never get better.” (These are her ANT’s - that stream spontaneously into her consciousness unbidden but which seem very real & plausible. These emerge early in Cognitive Therapy as you ask pt to identify thoughts associated with her feelings of low self-esteem & depression.) Case study formulation
Case study formulation • Now, consistent with above, & starting from infancy, childhood & adolescence let’s create a possible life history of early experiences (critical events, deprivations, parental personalities & peer relations, home, school & other experiences that may have shaped core beliefs & assumptions) _________________________________________________________________________________________________________________________________________________________ • Suggest core beliefs about her self, others & lifein general that arose from those experiences _________________________________________________________________________________________________________________________________________________________
Case study formulation • Propose schema & basic assumptions, standards, values, rules, guidelines for living that allow her to cope, despite core beliefs (remember “ if…then”, “should”, “must”, “ought”, “need” self-statements) _______________________________________________________________________________________________________________________________________________________________________________________ • Then, these protective views of her self, world & others begin to destabilise (rules are broken or assumptions are brought to fore), increasing her vulnerability to dysfunction, as one or more distressing situations develop, critical incidents occur, some repeated moderate or singular major upsets, adversities or catastrophes strike - such as _______________________________________________________________________________________________________________________________________________________________________________________
Case study formulation • A specific precipitating event triggers underlying maladaptive assumption or schema, or core belief & pt decompensates. In this case the event was ______________________________________________________________________________________________________ • Automatic negative thoughts – unwanted, intrusive, unhelpful thoughts & meanings unconsciously rooted in her core beliefs & schema then emerge uncontrollably, propelling her into therapy. Any variations on presenting ANT’s that might flow from our construction? ______________________________________________________________________________________________________ Italicized headings above are drawn from Aaron T. Beck’s Cognitive Therapy approach to case conceptualisation
Case study formulation Early experiences Formation of core beliefs about self, others, world & life in general Formation of schema & basic assumptions Critical incidents Precipitating event Automatic Negative Thoughts Armed with formulation based on above, you can more fully engage in Cognitive Therapy following steps outlined in slides 8 (Preparatory steps) & 15 – 17 (Managing ANT’s)
Patient & Therapist Resources • “Mind over Mood: a Cognitive Therapy Treatment Manual for Clients”. Greenberger, D., Padesky, C.A. New York Guilford Press 1995 (Workbook full of relevant exercises to help pts work thru problematic emotions) • “Reinventing your life: How to Break Free from Negative Life Patterns”. Young, JE & Klosko, J. Dutton, New York, 1993 (Helps pts identify schema & provides guidance on managing them) • “Cognitive Therapy Techniques – a practitioner’s guide”. Robert Leahy. NY Guilford Press 2003 (“A treasury of cognitive therapy strategies & techniques. All the tools a therapist needs . . .” Aaron T. Beck) • “Cognitive Therapy for Challenging Problems – What to do when the basics won’t work”. Beck, JS. NY Guilford Press 2005. (Suits novice & mature therapists alike)
Suggested responses • Now, consistent with above, & starting from infancy, childhood & adolescence let’s create a possible life history of early experiences (critical events, deprivations, parental personalities & peer relations, home, school & other experiences that may have shaped core beliefs & assumptions) • Distant father, suffers from depression, wanted son not daughter & repeatedly tells her so for years • Mother cold, aloof, can’t engage, so feelings of being unloved • Striving for approval through hard work, academically very successful & takes solace in that • Bullied at school relentlessly, told ‘ugly’, feelings of insecurity, sees world as hostile, demeaning, rejecting • Isolation, need for self-reliance & control, but desperate for others approval & sense of security
Suggested responses • Suggest core beliefs about her self, others & lifein general that arose from those experiences. (Remember - these are unconditional, absolutist core beliefs developing from early experiences) • “I am a failure, I am inadequate, I am worthless, I am unloved & unlovable, I shouldn’t have been born” • “I am alone, I am ugly & different from others. I cannot rely on others for anything” • “The world & others are hostile & they hate me”
Suggested responses • Propose schema & basic assumptions, standards, values, rules, guidelines for living that allow her to cope, despite core beliefs (remember “ if…then”, “should”, “must”, “ought”, “need” self-statements) • “If I try hard enough, others will grow to like me. I will get more affection. I need attention” • “If I am successful I will be approved of” • “If I show my inadequacies, others will reject me” • “If I can’t cope I will be seen as weak & helpless. Dependency is a sign of weakness” • “ If I am not loved & accepted I will always be unhappy”
Suggested responses • Then, these protective views of her self, world & others begin to destabilise, (rules are broken or assumptions are brought to fore) increasing her vulnerability to dysfunction, as one or more distressing situations develop, critical incidents occur, some repeated moderate or singular major upsets, adversities or catastrophes strike - such as • Experiences of rejection or disapproval that have cumulative effect • Bullying continues at university • Relationships break up • She has conflict with management at work about job conditions
Suggested responses • A specific precipitating event triggers underlying maladaptive assumption or schema, or core belief & pt decompensates. In this case the event was • Rejection by colleague at work • Automatic negative thoughts – unwanted, intrusive, unhelpful thoughts & meanings unconsciously rooted in her core beliefs & schema then emerge uncontrollably, propelling her into therapy. Any variations on presenting ANT’s that might flow from our construction? • As detailed in vignette Q & A