Download
1 / 65
660 likes | 765 Vues
IMQ Medical Staff and Hospital Collaboration in Performance Measurement and Quality Care May 20-21, 2005. American Heart Association “Get with the Guidelines” Implementation – A Generalizable Model. Timothy A. Denton, M.D., F.A.C.C. High Desert Heart Institute Victorville, CA. Outline.

E N D
IMQ Medical Staffand Hospital Collaborationin Performance Measurement and Quality CareMay 20-21, 2005 American Heart Association“Get with the Guidelines” Implementation– A Generalizable Model Timothy A. Denton, M.D., F.A.C.C. High Desert Heart Institute Victorville, CA
Outline • First Principles • The measurement of quality data • The use of quality data • Practical aspects • A specific implementation • Summary
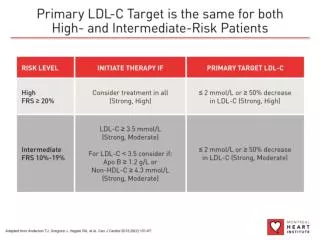
First Principles What are the goals of Medical Care? 1 - Prolong Survival 2 – Improve Quality-of-Life
First Principles Definition of Quality The degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge. Institute of Medicine (www.iom.edu)
First Principles ANOTHER Definition of Quality Provide those therapies that prolong survival and improve quality-of-life based on data from the medical literature. Institute of Medicine (www.iom.edu)
Example of Quality Care Many not in control of their diabetes, study says By The Associated Press Wednesday May 18, 2005 More than two-thirds of Americans with type 2 diabetes are not in control of their blood-sugar levels, according to a study released by the American Association of Clinical Endocrinologists today.
Example of Quality Care Program Tips Doctors for Healthy Patients FOX News Wednesday May 18, 2005 …If her diabetes stays under control, her doctor gets a cash bonus courtesy of a new program called Bridges to Excellence, designed to lower health-care costs…
Measurement of Quality Data • What should we measure? • How should we measure it?
Cardiac Surgery Reporting • Northern New England (1987) • New York (1989) • STS (1992) • Pennsylvania (1992) • VA NSQIP (1994) mort dec 27% • New Jersey (1994) • California (2001)
GOALS “…to give consumers information they can use in making informed choices…” “…to encourage hospitals to take an in-depth look at their cardiac surgery programs, and make changes that can improve surgical outcomes…” www.state.nj.us/health/hcsa/cabgs99/qna.htm
Types of Data • Mortality • Morbidity / Quality of Life • Process variables • Decision-making variables
Problems • Central Limit Theorem – The more you measure, the less you learn • Rare events – 2 % outcome characteristics are very difficult to stratify
Use of Quality Data • Who should use the data? • How should the data be used?
Who is the Audience? • Patients Where should I go for care? • Physicians How can I improve my care? • Government Do we intervene in care? • Administration Are we in compliance? • Payors To whom do we refer our insured?
HCFA Mortality Data • Mid to late 1980’s • Administrative database • Risk adjustment from same dataset • Poor accuracy • Rarely used by consumers • 31% of hospitals used for internal purposes • Ultimately discontinued JAMA. 1990;263:247-249 JAMA. 2000;283:1866-1874.
Medical Data Reporting • California CCMRP (CCORP) • California (patient opinions) • Maryland LOS, readmit, volume • New Jersey CABG reporting • New York CABG, PTCA Physician-specific • Pennsylvania Volume, Mortality, LOS 75 diagnostic groups • Texas Volume, Mortality 25 diagnostic groups • Virginia Volume, Mortality 25 diagnostic groups • South-Central Wisconsin Hip, Knee, cardiac Employer alliance • America’s Best Hospitals US News and World Reportwww.usnews.com • Guide to Hospitals Consumer Checkbookwww.checkbook.org • Hospital Report Cards Health Grades, Inc.www.healthgrades.com • JCAHO www.jcaho.org www.consumerreports.org
Cardiac Surgery Reporting • Excess mortality Not believed, cases reviewed • Excess mortality in high acuity patients MI<6 hrs, emergency • changed management of MI, NOT CABG Dzubian et al. Ann Thorac Surg 1999;58:1871-1876
Cardiac Surgery Reporting • Cardiac Surgeon survey • 70% no change in practice • Gaming of risk factors • Refused high risk patients because of reporting • “…denial of surgical treatment to high risk patients.” Burak et al. Ann Thorac Surg 1999;68:1195-1200
Practical Aspects • What systems of care exist now? • How can we develop new systems of care? • How can we develop efficient, new systems of care?
What systems are in place to assure optimal financial reimbursement?
Financial Screening Phone FAX email Web Patient Insurance Company Daily Charges Computer system Ward Accounts Payable Supplies Ledger Computer system Computer system Check emoney Bill Computer system ICD Coder Accounts Receivable Home
What systems are in place to assure optimal medical care?
Hmmmmm, did I forget anything? Clinician
A Specific Implementation Are there system examples that we can copy for optimizing medical care?
State Standings Ranked by CV indicators, mammog, immune, etc Jencks et al. JAMA 2000;284:1670
“Small” Committee • Chief of Cardiology • Clinical Chief of Cardiology • 2 Voluntary Staff • 2 Fulltime Staff • Cardiovascular specialist
A Committee of Stakeholders • All nurse managers • Dietary • Pharmacy • Cardiac rehab • Liaison nurses • Physician assistants • Fulltime staff • Voluntary staff
The Initial Questions What percentage of CSMC CAD patients have lipid levels on the chart? and what percentage are discharged on lipid-lowering medications?
Piper Seminole Checklist
Piper Seminole Checklist
Stakeholder Committee Ideas • Education • Change the system Pre-printed orders Better communication “tickler”
Pre-printed Orders • Admission to CCU • Post-cath • Transfer out of CCU • Transfer out of CSICU • Discharge instructions