Download
1 / 45
490 likes | 538 Vues
I nuovi antibiotici per la chemioterapia di precisione nella terapia delle infezioni da gram-negativi MDR. Francesco Menichetti, MD Professor of Infectious Diseases, University of Pisa Director, Infectious Diseases Department, Cisanello Hospital, Pisa

E N D
I nuovi antibiotici per la chemioterapia di precisione nella terapia delle infezioni da gram-negativi MDR Francesco Menichetti, MD Professor of Infectious Diseases, University of Pisa Director, Infectious Diseases Department, Cisanello Hospital, Pisa President, Italian Group for Antimicrobial Stewardship (GISA) www.antimicrobialstewardship.net
Disclosures 2017-2018 • Advisory Board: Angelini, MSD, Nordic Pharma • Speaker/chairman: Angelini, Astellas, Basilea, MSD, Pfizer • Events Sponsorship: Astellas, Gilead, MSD, BMS, Jansenn, ViiV, BioMerieux, Biotest, Becton-Dickinson, Nordic Pharma, Pfizer, Shionogi • Ongoing research protocol: Angelini, Astellas, Cidara, MSD, Shionogi, Theravance
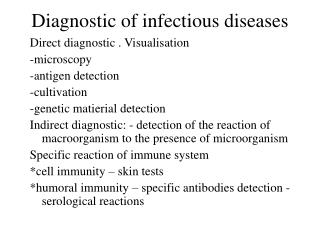
MDR gram-negative bacilli, resistance mechanisms & therapeutic options Pop-Vicas A & Opal SM Virulence 2013
Spectrum of β-lactamases carbapenemasi
Blood Isolates, Toscana 2015-2016 811 2087 ARS-SMART 2016
Treatment for ESBL infections The Sanford Guide 2018 • ESBL producingstrainssuspected by theirresistance in vitro • to Piperacillin, Cefotaxime, Ceftriaxone, Ceftazidime, Aztreonam • Life-threatening: • Carbapenems • Mild/moderate, non bacteremic, • low-inoculum, low MIC: • Cefepime • Piperacillin/tazobactam • Limited clinical data: • Ceftolozane/tazobactam • Ceftazidime/avibactam • UTI uncomplicated: FosfomycinNitrofurantoin
The MERINO Trial: piperacillin-tazobactam versus meropenem for the definitive treatment of bloodstream infections caused by third-generation cephalosporin non-susceptible Escherichia coli or Klebsiella spp • Adultpts from 32 sites in 9 countries(Singapore, Australia and Turkey). • Ptsincluded 378 (February 2014 to July 2017). • HAI: > 50% of the infections in the studygroup. • Urosepsis: 60.9% of the infections • E. coliresponsible of 86.5% of the cases Harris Pet al. ECCMID 2018 oralpresentation
MERINO trial: preliminaryresults Harris Pet al. ECCMID 2018 oralpresentation
The MERINO Trial: piperacillin-tazobactam versus meropenem for the definitive treatment of bloodstream infections caused by third-generation cephalosporin non-susceptible Escherichia coli or Klebsiella spp • No differencebetween the twogroupsregardingsubsequentinfections of drug-resistantbacteria or C. difficile, butdifference in mortality rate wassignificant. • Twenty-threepatients(12.3%) treated with pip-tazodied by the 30-day markcompared with sevenpatients(3.7%) whohadbeentreated with meropenem. • Pip-tazowassignificantlylesseffectivethan MPN for potentiallyfatal BSI caused by ceftriaxone-resistantE. coli and K. pneumoniae and should be avoided Harris Pet al. ECCMID 2018 oralpresentation
The domino effect of the ESBL pandemic Dissemination of Enterics producing ESBLs Carbapenem-sparing regimens ? Carbapenem Overuse Dissemination of Carbapenem R Gram-negatives Idea: Gianni Rossolini
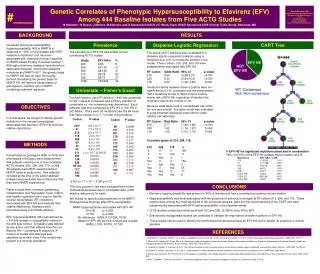
335 pts included; 249 received empiric CPSs and 86 OADs. • Most frequent OADs were AGs (43 pts) and FQs (20 pts). • Empiric therapy with OADs was not associated with increased mortality. • OADs were neither associated with 14-day clinical failure nor increased length of hospital stay. • This information allows more options to be considered for empiric therapy, at least for some patients, depending on ocal susceptibility patterns of ESBL-E.
Early administration of OADs for BSI due to ESBL-E does not seem to compromise outcome in comparison with carbapenems, and might be an option for empiric regimens for many patients, depending on local susceptibility patterns. • This may be particularly applied to the use of aminoglycosides in urinary tract sepsis potentially caused by ESBL-Eand would justify the design of a randomized trial; • However, until more data are available, we would still recommend considering carbapenems (or BL-BLI) for patients at risk of ESBL-E presenting with septic shock or with a non–urinary tract source of sepsis.
Ceftolozane demonstrates good activity against Enterobacteriaceae but its activity is limited against ESBLs. • Tazobactam is a potent, irreversible inhibitor of most ESBLs. • The MIC50/MIC90 of this agent for ESBL-producing E. coli are 0.5/4 μg/mL and for K. pneumoniae 4/>32 μg/mL • Differences in MIC distributions may be reflective of discrepancies in ESBL genes present. • The blaCTX-M genes predominate in E. coli, whereas there is often a preponderance of blaTEM/SHV in K. pneumoniae, with variations in local epidemiology.
Ceftolozane-tazobactam(in combination with metronidazole) wascompared to meropenem for the treatment of complicated intra-abdominalinfections in phase 2 and phase 3 trials thatincluded4 and 50 people, respectively, with ESBL-producingEnterobacteriaceae. • Although the limitednumber of ESBLsprecluded a robustanalysis, this compound performedsimilarlyagainst ESBL-producing and non-ESBL producingisolates.
Efficacy of ceftolozane/tazobactam against urinary tract and intra-abdominal infections caused by ESBL-producing Escherichia coli and Klebsiella pneumoniae: a pooled analysis of Phase 3 clinical trials At ceftolozane/tazobactam concentrations ≤2 mg/L, 95% of ESBL-E. coli and 56.7% of ESBL- K. pneumoniae were inhibited Popejoy M, J Antimicrob Chemother, 2017; 72: 268-72
Ceftazidime-avibactam is usually more active in vitro against ESBL producers than ceftolozane-tazobactam. • The MIC50/MIC 90 for ESBL-producing E. coli are 0.12/0.25 μg/mL and for K. pneumoniae 0.5/1 μg/mL • Phase 2/3 studies compared ceftazidime-avibactam (plus metronidazole) vs meropenem for intra-abdominal infections, but did not specifically compare outcomes of ESBL-confirmed pathogens. • Data from a phase 3 study comparing ceftazidime-avibactam and doripenem in UTIs showed similar microbiological response for ceftazidime-resistant Enterobacteriaceae, most of which were ESBL producers
Carbapenem-resistantenterobacteriaceae (CRE): definition • CRE was defined as an Enterobacteriaceae isolate demonstrating resistance to any carbapenem (ertapenem, meropenem, imipenem, and/or doripenem), based upon antimicrobial susceptibility testing (AST). • Carbapenem resistance was defined as an Ertapenem MIC ≥2 mcg/ml and MPN and/or IP MIC ≥4 mcg/ml. Clinical Infectious Diseases Advance Access published November 9, 2016
Meropenem use for CRE: MIC, please • For Meropenem MICs of ≤4 mcg/ml: standard-infusion of 2 grams t.i.d. considered active, based on existing pK/pD studies. • For Meropenem MICs of 8 mcg/ml: extended-infusion (2 grams t.i.d. over at least 3 hours) potentially active. • Modeling of extended-infusion strategies suggest that reasonable target attainment can be anticipated with meropenem MICs of up to 8 mcg/ml, and possibly 16 mcg/ml Clinical Infectious Diseases Advance Access published November 9, 2016
The double domino effectof the CRE epidemic Dissemination of CRE Further Carbapenem Overuse Colistin overuse Dissemination of Colistin R strains
K. pneumoniae Col-R, 2015- 2016 Col-R: 8,1%
Comparing the Outcomes of Patients with Carbapenemase-Producing and Non-Carbapenemase-Producing Carbapenem-Resistant Enterobacteriaceae Bacteremia • Carbapenem-resistantEnterobacteriaceae (CRE) bacteremiaisassociated with mortality up to 60%. • Carbapenemresistance can be mediated via: carbapenemase production (CP-CRE) or • production of ESBLs and/or AmpCcephalosporinasescombined with altered membrane permeability(non-CP-CRE). • Need to know the outcomesassociated with CRE bacteremiaaccording to underlyingresistancemechanisms. Clinical Infectious Diseases Advance Access published November 9, 2016
Comparingthe Outcomes of Patients with Carbapenemase-Producing and Non-Carbapenemase-ProducingCarbapenem-ResistantEnterobacteriaceaeBacteremia • In a cohort of 83 CRE bacteremic patients, the odds of dying within 14 days were four times greater for carbapenemase-producing (CP) CRE compared with non-CP-CRE patients, adjusting for severity of illness, underlying medical conditions, and differences in antibiotic regimens. Clinical Infectious Diseases Advance Access published November 9, 2016
Expanded spectrum of β-lactamase inhibition J Antimicrob Chemother 2016; 71:2713-22
Ceftazidime – Avibactam • Spectrum of activity: Gram-negatives, including MDR P. aeruginosa,ESBL-producing strains, KPC-Kp • EMA approval in June 2016 • c-UTI, including Pyelonephritis • C-IAI (plus metronidazole) • Nosocomial pneumonia • Gram-neg. infection with limited treatment option • IV dose: 2.5 g (2 g ceftazidime; 0.5 g avibactam) q8h (2-h infusion)
Ceftazidime/avibactampotentialdrawbacks • The development of resistance to CAZ/AVI (MIC ≥16 mg/L) was observed following relatively short courses of therapy. • Reducing the development of resistance by using a combination therapy approach ? • Early development of resistance a unique flaw of CAZ/AVI or might it be seen with other new βL-βLIs combinations ? • Much of the resistance reported seen in K. pneumoniae isolates, how common will this phenotype in non- Klebsiellae spp. harbouring KPCs ? • In geographical areas where MBLs are observed at higher rates, what is the overall utility of ceftazidime/avibactam in clinical practice ?
Aztreonam/Avibactam • Aztreonam • Non gravato da reazioni allergiche crociate con altri β-lattamici (eccetto ceftazidime) • Idrolizzato da ESBL, AmpC e • KPC • NON idrolizzato da MBLs • Avibactam • Inibitore non β-lattamico • NON Idrolizzato da: • ESBL • AmpC β-lattamasi • KPC Aztreonam Ceftazidime/Avibactam Falagas M.E. Expert Review 2016
Imipenem/Relebactam • Relebactam (MK7655) is a piperidine analogue diazabicyclooctane beta-lactamase inhibitor designed to have inhibitory activity against class A and class C beta-lactamases. • In KPC-producing K. pneumoniae the addition of relebactam resulted in lowering imipenem MICs by up to 64-fold. • More modest potentiation was seen with other ESBL- and AmpC producing strains. • Little or no reduction was seen in OXA-48-producing K. pneumoniae or OXA-23-producing A. baumannii, suggesting relebactam, unlike avibactam, does not have significant activity against class D enzymes • Imipenem MICs were reduced from ≥16 mg/L to 2 mg/L in the presence of relebactam when imipenem-resistant P. aeruginosa isolates were tested.
Meropenem/Vaborbactam • Vaborbactam is a novel cyclic boronic acid inhibitor of many class A, class C and some class D beta-lactamases. • Vaborbactam acts via the creation of a covalent (dative) bond between its boron moiety and the serine hydroxyl of beta lactamase. • The addition of vaborbactam at 8 μg/ml to meropenem resulted in ≥ 16-fold reduction in MICs for KPC producing E. coli, K. pneumoniae, and Enterobacter spp. isolates. • In a limited number of strains, the combination appeared to have reduced activity against KPC-producing K.pneumoniae isolates with diminished expression of porin genes ompK35 and ompK36. • Little effect on A. baumannii containing OXA-type carbapenemases or P. aeruginosa was observed
Cefiderocol • Cefiderocolisa siderophorecephalosporinantibiotic with a catecholmoiety on the 3-position side chain. • The catechol side chainenablesferricironionbinding, and the resultingcomplexisactivelytransportedintobacteria via ferricirontransportersystems with subsequentdestruction of cellwall. • Cefiderocolhasbeenshown to be potent in vitro againstgram-negative organisms, includingCRE and MDR P. aeruginosa and A. baumannii. • Thisactivityisconsidered to be due to the efficientuptake via the activesiderophoresystemsand alsoto the high stability of cefiderocolagainst CPS hydrolysis.
Terapia mirata carbapenem-sparing in infezioni gravi da gram-neg
Conoscere i nuovi antibiotici: un dovere per il clinico • …..ed un’opportunità per i pazienti……. • Curiosità, non pigrizia prescrittiva • Modello di stewardship condivisa • Raccomandazioni terapeutiche condivise • Gestione della scheda AIFA • Ruolo armonico delle società scientifiche • Sistema nazionale delle LG (ISS) www.antimicrobialstewardship.net
www.antimicrobialstewardship.net Presidente Onorario: Prof. Johnatan Cohen Società Scientifica multidisciplinare, promuove la cultura dell’ASP intesa come GOVERNO CLINICO DELLA TERAPIA ANTIMICROBICA attraverso il confronto equo tra esperti e prescrittori.