Download
1 / 30
420 likes | 815 Vues
Brain Arteriovenous Malformations in Adults. Eric Johnson OHSU MS3 12/14/07. The story of AVMs is an interesting one, because. Although rare, they can be fatal Some AVMs are discovered incidentally in asymptomatic individuals

E N D
Brain Arteriovenous Malformations in Adults Eric Johnson OHSU MS3 12/14/07
The story of AVMs is an interesting one, because . . . • Although rare, they can be fatal • Some AVMs are discovered incidentally in asymptomatic individuals • Our treatment modalities for AVMs have evolved faster than our knowledge about their incidence, prevalence and natural history
Widely accepted surgical treatments have significant risks (neurological deficits, death) • There are no prospective, randomized trials comparing surgical treatments to conservative medical treatments, or even no treatment (a control population) • However, many (most?) AVMs are treated surgically (even in asymptomatic individuals) More about this later . . .
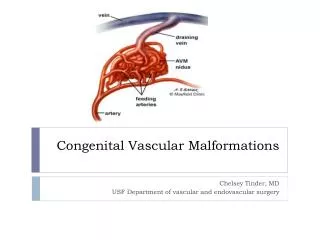
Definition of an AVM • A congenital shunt between the arterial and venous systems • A tangle of abnormal vessels (nidus) • Vary in size and location http://neuro.wehealny.org/endo/illus/13_01.gif
Epidemiology and Natural History (These figures are debated in the literature) • Incidence: about 1 per 100,000 per year • Point prevalence: about 18 per 100,000 • AVMs account for: • 1-2% of all strokes • 9% of subarachnoid hemorrhages • Annual risk of hemorrhage from unruptured AVM: about 2% (poor data) • Risk of recurrent hemorrhage: up to %18 in the first year, uncertain thereafter (poor data) • Annual case fatality: 1-1.5% (poor data) (Al-Shahi et al.)
Pathogenesis • Poorly understood • Genetic variation may play a role (Hashimoto et al.)
Pathology • AVMs divert blood flow from surrounding brain parenchyma • This leads to areas of chronic ischemia, producing gliotic tissue • AVM vessels have abnormal internal elastic lamina and/or media, making them prone to rupture Kumar et al.
Clinical Presentation • Most commonly present before age 40, some with more than one symptom: • 53% hemorrhage • 30% generalized seizure • 14% chronic headache • 10% focal seizures • 7% persistent neurological deficits • 5% progressive neurological deficits • About one-fifth are discovered incidentally in asymptomatic individuals Hofmeister et al. Al-Shahi and Warlow
Diagnosis • Diagnosis is made or confirmed by diagnostic imaging • Angiography is considered the “gold standard” for diagnosis and treatment planning • However, there is very little data about the sensitivity and specificity, as well as intra- and inter-observer variability of imaging modalities used to diagnose and classify AVMs
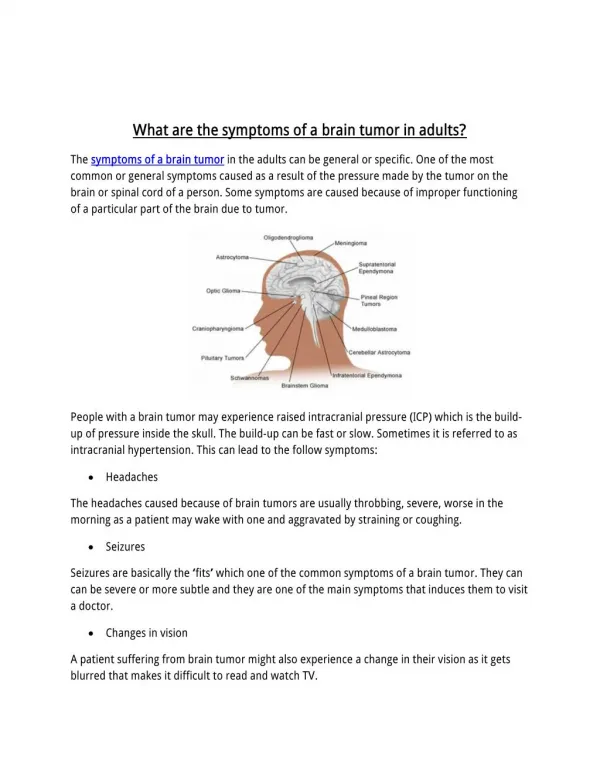
CT Imaging • What to look for: • Vascular tangles that are serpiginous and possibly hyperdense, due to the pooling of blood • May contain punctate or curvilinear calcifications • AVMs will enhance with contrast • An AVM may present as a hemorrhage
Axial CT without contrast Al-Shahi et al.
Axial CT with contrast Al-Shahi et al.
Axial CT with hemorrhage secondary to AVM http://www.brain-aneurysm.com/images/avm_pageimages/3.jpg
MRI Imaging • What to look for: • Curvilinear flow-voids
Coronal, unenhanced, T1- weighted MRI Al-Shahi et al.
Saggital, T1-weighted MRI http://www.hmc.psu.edu/neurosurgery/services/images/LF1.jpg
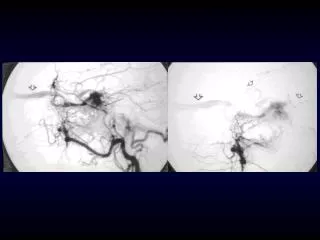
Angiography • What to look for: • The three components of an AVM: • Enlarged feeding artery • Core/nidus • Enlarged draining vein • Early venous filling during the arterial phase of enhancement
Cerebral angiogram ICA: Internal carotid artery MCA: Middle cerebral artery DV: Draining vein Arrows: AVM nidus http://www.brain-aneurysm.com/images/avm_pageimages/4.jpg
Cerebral angiogram http://www.ucl.ac.uk/medical-modelling/myimages/Figure1.jpg
Treatment • Surgical options include: • Neurosurgery (resect the AVM) • Sterotactic radiosurgery (ablate the AVM through direct radiation, which causes thrombosis over time) • Endovascular embolization (ablate AVM through direct thrombosis with embolic material) • A combination of these modalities • AVMs are graded in an effort to help guide treatment decisions. The most common grading system is the Spetzer-Martin Scale:
Spetzler-Martin AVM Grading Scale • Size • 0-3 cm 1 • 3.1-6.0 cm 2 • >6 cm 3 • Location • Noneloquent 0 • Eloquent 1 • Deep venous drainage • Not present 0 • Present 1 * Eloquent brain regions can be defined as “sensorimotor, language, and visual cortex; the hypothalamus and thalamus; the internal capsule; the brain stem; the cerebellar peduncles; and the deep cerebellar nuclei.” (Hofmeister et. al) Grading scale adapted from Ogilvy et al.
Neurosurgery • Primarily for Spetzler-Martin grade 1 and 2 lesions (Ogilvy et al.) • For complications, one study reported that 8% of patients either had a persistent neurological deficit or died as a result of surgery (Mohr et al.)
Stereotactic Radiosurgery • Primarily for small AVMs, especially in eloquent brain locations (Ogilvy et al.) • Friedman et al. reported the following complication rates: • 10% post-treatment hemorrhage • 3.7% transient radiation-induced complication • 1% permanent radiation-induced complication
Endovascular Embolization • Primarily a presurgical modality for large cortical AVMs to reduce nidus size (Ogilvy et al.) • “Palliative embolization may be used in large nonsurgical or nonradiosurgical AVMs” (Ogilvy et al.) • Complication rate (Mohr et al): • Morbidity: 13% • Mortality: 2%
Some quotes from UpToDate: • “Surgery is the mainstay of treatment; radiosurgery is a useful option . . . and endovascular embolization has become a useful adjunct to these techniques.” • “There is no evidence from randomized clinical trials to guide treatment decisions.” • “There are no randomized controlled trials of radiosurgery for brain AVMs, and none are likely to be performed as the benefit of radiosurgery for radiographic obliteration of brain AVMs is widely accepted.” (Singer et al.)
From the Cochrane Collaboration: “There is no clear evidence from randomised trials with clear clinical outcomes, comparing different interventional treatments for brain AVMs against each other or against usual medical therapy, to guide the interventional treatment of brain AVMs in adults.” (Al-Shahi and Warlow)
But there’s hope . . . • A Randomized Trial of Unruptured Brain AVMs (the ARUBA trial) is currently recruiting participants: • “[Current] treatments are administered on the assumption that they can be achieved at acceptably minor complication rates, decrease the risk of subsequent hemorrhage, and lead to better long-term outcomes.” • Therefore, the “purpose of this study is to determine if medical management is better than invasive therapy for improving the long-term outcome of patients with unruptured brain arteriovenous malformations.” http://clinicaltrials.gov/ct/show/NCT00389181?order=2
Summary • Because AVMs are rare, little is understood about their epidemiology and natural history • Because they cause significant morbidity and mortality, they are often treated • Commonly used treatments for AVMs also cause significant morbidity and mortality • Patients are being treated in the absence of a sufficient cost-benefit analysis regarding those treatments
We need more research on classifying AVMs based on radiological findings that are consistent and reproducible among radiologists • We also need more research comparing treatments to a control population and to each other for different classes of AVMs • Stay tuned for the results of the ARUBA Trial!
Bibliography Al-Shahi et al. “A systematic review of the frequency and prognosis of arteriovenous malformation of the brain in adults.” Brain. 2001; 124:1900-1926. Al-Shahi R, Warlow CP. Interventions for treating brain arteriovenous malformations in adults. Cochrane Database of Systematic Reviews 2006, Issue 1. Art. No.: CD003436. DOI: 10.1002/14651858.CD003436.pub2. Friedman, et al. “Analysis of factors predictive of successor complications in arteriovenous malformation radiosurgery.” Neurosurgery. 2003; 52:296-308. Hashimoto et al. “Gene microaray analysis of human brain arteriovenous malformations. Neurosurgery. 2004; 54:410. Hofmeister et al. “Demographic, Morphological, and Clinical Characteristics of 1289 Patients With Brain Arteriovenous Malformation.” Stroke. 2000; 31:1307-1310. Kumar et al. Pathologic basis of Disease, 7th Edition. Elsevier Saunders: Philadelphia, PA. 2005. Mohr et al. “Arteriovenous malformations of the brain in adults.” NEJM. 1999; 230:1812-1818. Ogilvy et al. “Recommendations for the Management of Intracranial Arteriovenous Malformations” Stroke. 2001; 32:1458-1471. Singer et al. “Brain arteriovenous malformations.” UpToDate Online 2007. The ARUBA Trial. <http://clinicaltrials.gov/ct/show/NCT00389181?order=2>