Download
1 / 27
280 likes | 322 Vues
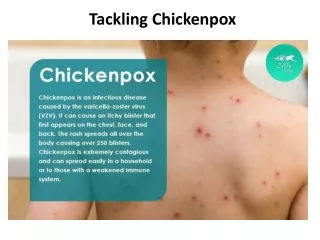
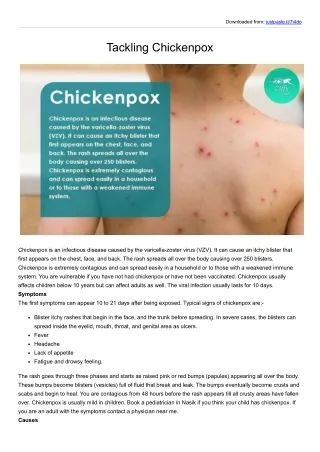
Varicella Chickenpox. Dr hab. n. med. Ewa Majda-Stanislawska. Varicella-zoster virus (VZV) causes two distinct clinical diseases: 1. Varicella, more commonly called chickenpox: is the primary infection results from exposure of a person susceptible to the virus

E N D
Varicella Chickenpox Dr hab. n. med. Ewa Majda-Stanislawska
Varicella-zoster virus (VZV) causes two distinct clinical diseases: 1. Varicella, more commonly called chickenpox: is the primary infection results from exposure of a person susceptible to the virus 2. Herpes zoster is due to the recurrence of infection is more localized often referred to as shingles, is a common infection among the elderly.
Shingles has been recognized since ancient times as a unique clinical entity because of the dermatomal vesicular rash Chickenpox was often confused with smallpox
VZV is a member of the Herpesviridae family The virus has icosapentahedral symmetry It contains centrally located double-stranded DNA with a surrounding envelope. Only enveloped virions are infectious; this may account for the lability of VZV. The envelope is sensitive to detergent, ether, and air drying.
Humans are the only known reservoir for VZV. Chickenpox is a common infection of childhood and affects both genders equally and people of all races. It becomes epidemic among susceptible persons during seasonal periods: late winter and early spring close contact appears to be the key determinant for transmission
90% of cases occur in children younger than 13 years Approximately 10% of persons older than 15 years are considered susceptible to VZV infection. The incubation period of chickenpox is generally regarded to be 14 to 15 days, but disease can appear within a range of 10 to 20 days
Infectivity Patients are infectious for a period of approximately 48 hours before the period of vesicle formation for 4 to 5 days thereafter until all vesicles are crusted.
Herpes zoster VZV characteristically becomes latent after primary infection within the dorsal root ganglia. Reactivation leads to herpes zoster, a sporadic disease. Herpes zoster is a disease that occurs at all ages, but it afflicts about 20% or more of the population overall, mainly the elderly.
Herpes zoster, occurs in persons who are seropositive for VZV or, more specifically, in those who have had chickenpox. Reactivation appears to be dependent on a balance between virus and host factors Persons who are immunocompromised have a higher incidence of both chickenpox and shingles. Herpes zoster occurs within the first 2 years of life in children born to women who have had chickenpox during pregnancy. These cases probably reflect in utero chickenpox with reactivation early in life.
Mortality rate of varicella There have been approximately 250 deaths per year in the USA. For the normal child, chickenpox-associated mortality is less than 2 per 100,000 cases. This risk increases by more than 15-fold for adults
Manifestations of chickenpox are a rash, low-grade fever, and malaise. A prodrome of symptoms may occur 1 to 2 days before the onset of the exanthem in a few patients. For the most part, chickenpox in the immunocompetent child is a benign illness associated with a temperature of 37 -38oC of 3 to 5 days' duration
The skin manifestations consist of maculopapules, vesicles, and scabs in varying stages of evolution. The lesions initially contain clear vesicular fluid, over a very short period of time they pustulate and scab. Most lesions are small, having an erythematous base with a diameter of 5 mm to as large as 12 to 13 mm.
The lesions can be round or oval; central umbilication occurs as healing progresses. If they do not rupture within a few hours, the contents rapidly become purulent in appearance. The lesions appear on the trunk and face, and rapidly spread centrifugally to involve other areas of the body. Successive crops of lesions generally appear over a period of 2 to 4 days.
Early in the disease, the hallmark of the infection is the appearance of lesions at all stages The lesions can also be found on the mucosa of the oropharynx and even the vagina. The crusts completely fall off within 1 to 2 weeks after the onset of infection and leave a slightly depressed area of skin.
Complications - skin bacterial superinfection: often due to gram-positive organisms. Streptococcal toxic shock is a rare but potentially lethal complication of varicella. infection in the neutropenic host can be systemic.
Complications - CNS involvement acute cerebellar ataxia or encephalitis. Cerebellar ataxia has been estimated to occur in 1 in 4000 cases among children younger than 15 years. It can appear as late as 21 days after the onset of rash. Usually it presents within 1 week of the onset of the exanthem.
Cerebellar ataxia - symptoms Ataxia, vomiting, altered speech, fever, vertigo, tremor. Cerebrospinal fluid (CSF) demonstrates lymphocytosis and elevated levels of protein.
Complications - encephalitis Encephalitis is reported to occur in 0.1% to 0.2% of persons with the disease. It is characterized by depression in the level of consciousness with progressive headaches, vomiting, altered thought patterns, fever, frequent seizures. The duration of disease in these patients is at least 2 weeks. Some patients experience progressive neurologic deterioration that leads to death. Mortality in patients who develop encephalitis has been estimated to range between 5% and 20%, neurologic sequelae occur in as many as 15% of survivors.
Complications - varicella pneumonitis Occurs more commonly in adults and in immunocompromised persons It appears 3 to 5 days into the course of illness I is associated with: tachypnea, cough, dyspnea, fever. Chest radiographs usually reveal nodular or interstitial pneumonia. Varicella pneumonitis can be life threatening when it occurs in pregnant women during the second or third trimester
Perinatal varicella high death rate when maternal disease develops: 5 days before delivery or up to 48 hours postpartum. This is the consequence of the newborn failing to receive protective transplacental antibodies as well as the immaturity of the neonatal immune system. The mortality has been reported to be as high as 30%. Affected children have progressive disease involving visceral organs, especially the lung.
Congenital varicella, rather uncommon, Characterized by: skin scarring, hypoplastic extremities, eye abnormalities, evidence of CNS impairment
Varicella has been associated epidemiologically with the development of Reye's syndrome and coadministration of aspirin Therefore, the administration of aspirin is contraindicated in persons with varicella.
The diagnosis of both chickenpox and shingles is usually made by history and physical examination
Treatment The medical management of chickenpox and shingles in the normal host is directed toward reduction of complications. For chickenpox, hygiene is important: bathing, astringent soaks, closely cropped fingernails to avoid a source for secondary bacterial infection associated with scratching of the pruritic skin lesions. .
Oral treatment with Acyclovir In normal children, adolescents, and adults shortens the duration of lesion formation by about 1 day, reduces the total number of new lesions by approximately 25%, diminishes constitutional symptoms in one third of patients. Therapy for high-risk groups of patients: premature infants, children with bronchopulmonary dysplasia within 24 hours of onset of disease. In children 2 to 16 years old, the oral dosage is 20 mg/kg 4 times daily for 5 days (maximum of 800 mg daily). Adolescents and adults can receive up to 800 mg 5 times a day.
Parenteral treatment with Acyclovir The recommended dosage is from 5 to 10 mg/kg administered intravenously every 8 hours or, as suggested by some, 500 mg/m2 intravenously every 8 hours, especially for children. Indications: immunocompromised host, neurological complications. pneumonitis