Download
1 / 1
10 likes | 108 Vues
No. 025. Ductal Adenocarcinoma of the prostate: A marker of high volume, high stage disease. Marlon Perera 1 , Damien Bolton 2 and David Clouston 3 1 Western General Hospital, Footscray , VIC

E N D
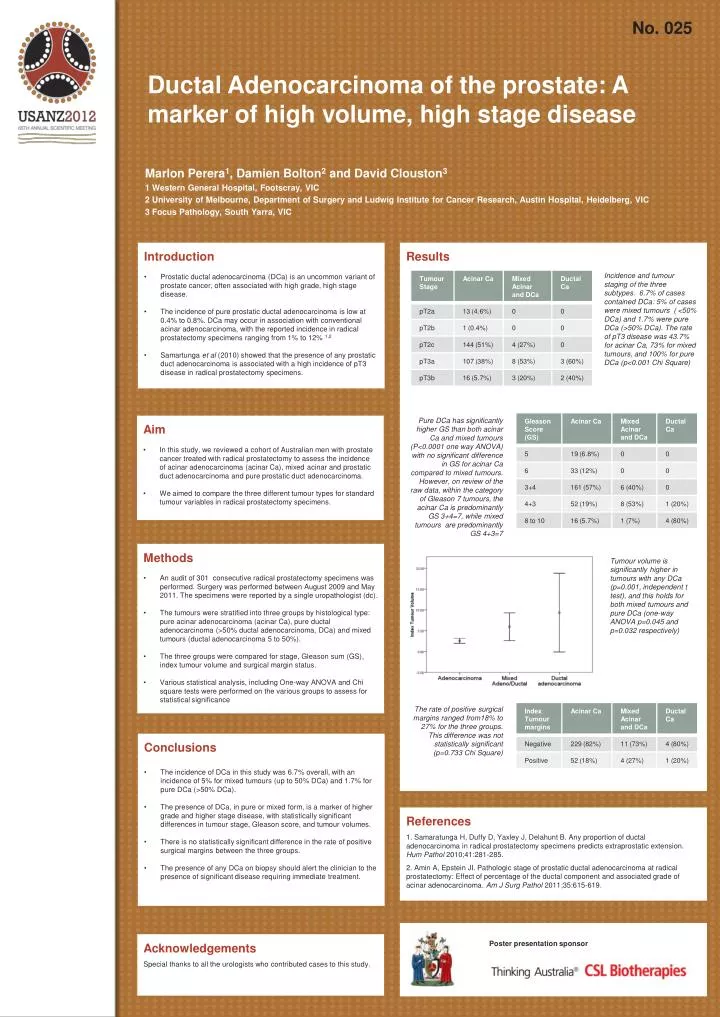
No. 025 Ductal Adenocarcinoma of the prostate: A marker of high volume, high stage disease Marlon Perera1, Damien Bolton2 and David Clouston3 1 Western General Hospital, Footscray, VIC 2 University of Melbourne, Department of Surgery and Ludwig Institute for Cancer Research, Austin Hospital, Heidelberg, VIC 3 Focus Pathology, South Yarra, VIC • Introduction • Prostatic ductal adenocarcinoma (DCa) is an uncommon variant of prostate cancer, often associated with high grade, high stage disease. • The incidence of pure prostatic ductal adenocarcinoma is low at 0.4% to 0.8%. DCa may occur in association with conventional acinar adenocarcinoma, with the reported incidence in radical prostatectomy specimens ranging from 1% to 12% 1,2 • Samartungaet al (2010) showed that the presence of any prostatic duct adenocarcinoma is associated with a high incidence of pT3 disease in radical prostatectomy specimens. Results Incidence and tumour staging of the three subtypes. 6.7% of cases contained DCa: 5% of cases were mixed tumours ( <50% DCa) and 1.7% were pure DCa (>50% DCa). The rate of pT3 disease was 43.7% for acinar Ca, 73% for mixed tumours, and 100% for pure DCa (p<0.001 Chi Square) Pure DCa has significantly higher GS than both acinar Ca and mixed tumours (P<0.0001 one way ANOVA) with no significant difference in GS for acinar Ca compared to mixed tumours. However, on review of the raw data, within the category of Gleason 7 tumours, the acinar Ca is predominantly GS 3+4=7, while mixed tumours are predominantly GS 4+3=7 • Aim • In this study, we reviewed a cohort of Australian men with prostate cancer treated with radical prostatectomy to assess the incidence of acinar adenocarcinoma (acinar Ca), mixed acinar and prostatic duct adenocarcinoma and pure prostatic duct adenocarcinoma. • We aimed to compare the three different tumour types for standard tumour variables in radical prostatectomy specimens. • Methods • An audit of 301 consecutive radical prostatectomy specimens was performed. Surgery was performed between August 2009 and May 2011. The specimens were reported by a single uropathologist (dc). • The tumours were stratified into three groups by histological type: pure acinar adenocarcinoma (acinar Ca), pure ductal adenocarcinoma (>50% ductal adenocarcinoma, DCa) and mixed tumours (ductal adenocarcinoma 5 to 50%). • The three groups were compared for stage, Gleason sum (GS), index tumour volume and surgical margin status. • Various statistical analysis, including One-way ANOVA and Chi square tests were performed on the various groups to assess for statistical significance Tumour volume is significantly higher in tumours with any DCa (p=0.001, independent t test), and this holds for both mixed tumours and pure DCa (one-way ANOVA p=0.045 and p=0.032 respectively) The rate of positive surgical margins ranged from18% to 27% for the three groups. This difference was not statistically significant (p=0.733 Chi Square) • Conclusions • The incidence of DCain this study was 6.7% overall, with an incidence of 5% for mixed tumours (up to 50% DCa) and 1.7% for pure DCa (>50% DCa). • The presence of DCa, in pure or mixed form, is a marker of higher grade and higher stage disease, with statistically significant differences in tumour stage, Gleason score, and tumour volumes. • There is no statistically significant difference in the rate of positive surgical margins between the three groups. • The presence of any DCa on biopsy should alert the clinician to the presence of significant disease requiring immediate treatment. • References • 1. Samaratunga H, Duffy D, Yaxley J, Delahunt B. Any proportion of ductal adenocarcinoma in radical prostatectomy specimens predicts extraprostatic extension. Hum Pathol2010;41:281-285. • 2. Amin A, Epstein JI. Pathologic stage of prostatic ductal adenocarcinoma at radical prostatectomy: Effect of percentage of the ductal component and associated grade of acinar adenocarcinoma. Am J Surg Pathol2011;35:615-619. Acknowledgements Special thanks to all the urologists who contributed cases to this study. Poster presentation sponsor