Download
1 / 15
150 likes | 226 Vues
THE EFFECT OF MEDICAID RATE ON POTENTIALLY PREVENTABLE HOSPITALIZATIONS FROM NURSING HOME *. Orna Intrator with V. Mor, N. Wu, D. Grabowski † , D. Gifford and Z. Feng Brown University and † UAB. * Funded by NIA RO1 AG20557. Objective.

E N D
THE EFFECT OF MEDICAID RATE ON POTENTIALLY PREVENTABLE HOSPITALIZATIONS FROM NURSING HOME* Orna Intrator with V. Mor, N. Wu, D. Grabowski†, D. Gifford and Z. Feng Brown University and † UAB * Funded by NIA RO1 AG20557
Objective • Medicaid payment rates are reflected in the availability of the clinical and managerial infrastructure necessary to manage nursing home residents’ medical conditions. • Over 60% of all nursing home residents are Medicaid recipients • Differences in reimbursement rates and other Medicaid reimbursement policies likely to contribute to observed inter-state differences in hospitalization rates.
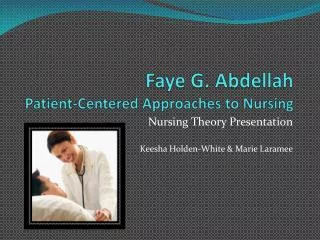
STATE Policies MARKET Context NURSING HOME Context Hospitalization RESIDENT Characteristics CONCEPTUAL MODEL Direct and indirect effects
Hypotheses: direct effects • Nursing home residents in states with • Higher Medicaid rates experience fewer potentially preventable hospitalizations. • Bedhold policies will be more likely to be hospitalized • With casemix reimbursement will be more likely to be hospitalized because a hospitalization would result in change in per-diem rate
Hypotheses: Indirect effects • Higher Medicaid rates • More NP/PAs • Less hospitalizations • More RNs in nursing home nursing force • Less hospitalizations • More investment in physicians • Less hospitalizations
Data and Cohort • Minimum Data Set (MDS) to identify long-stay residents or urban free standing nursing homes in 48 contiguous states in 2000 (N=575,188 in 9124 facilities) • Facility data from Centers for Medicare and Medicaid Services’ Online Survey Certification and Reporting (OSCAR) system. • Medicare claims of all hospitalizations within 5 months of baseline MDS that were initiated from baseline nursing home (N=101,105) • Area Resource File for information on counties as NH markets
Survey of State Medicaid Policies* • 48 continguous states contacted • Information on: • Method of calculation • Casemix method and updating schedule • Average per-diem payment rate and ancillary payments • Bedhold rate and durations • CON and moratorium *Forthcoming article in Health Affairs Web Exclusive June 18, 2004
State Policy Measures • Average per diem rate: • Total payments divided by total bed days • Free standing and hospital based • Annually, 1999-2002 • Used 2000 data in this study • Bedhold policies* • Proportion of NH rate paid • Maximum number days in period • Minimum occupancy requirements *Poster at 6pm tonight
State Policy Measures • Casemix reimbursement: • Type of system (RUG based, other) • How frequently updated (annually, quarterly) • Based on resident, facility, or both • Four category variable: • No casemix (N=17) • Not resident specific only updated annually (N=9) • Facility specific quarterly or semi-annually (N=14) • Most responsive: Resident specific quarterly or semi-annually or both and quarterly (N=8)
Outcome Definition • Hierarchical outcome: • Any potentially preventable hospitalization (using ambulatory care sensitive diagnoses) • Any other hospitalization • Death • Remaining in the facility. Distribution of outcome: Any potentially preventable …………… 7.4% Other Hosp ……………………………..……. 12.6% Died ……………………………………….……….. 9.2%
Model and Estimation • Multinomial response (4 categories) • Multilevel: • Resident • Facility • County • State • Estimation using MLWiN for binomial response: Outcome vs. remain in NH
Policy Implications • Highlights competing motivation of Medicaid and Medicare: • Higher Medicaid rates lower Medicare expenditures from less hospitalizations higher Medicare expenditures from increased LOS • Higher bedhold rates higher Medicare expenditures • More bedhold days better quality of life • What is “optimal” policy • For Medicare? For Medicaid? For Residents?