Download
1 / 1
10 likes | 69 Vues
TABLE 1 Description of the 88 HIV-infected pediatric patients included in the study. Sex (Boys/Girls) 43/45 Age (years) 13.9 (0.5) a Weight (kg) 45.8 (1.7) a Height (cm) 151.5 (2.1) a BMI (kg/m 2 ) 19.2 (0.4) a Pubertal development (n) Stage I: 20 Stages II-III: 22 Stages IV-V: 45

E N D
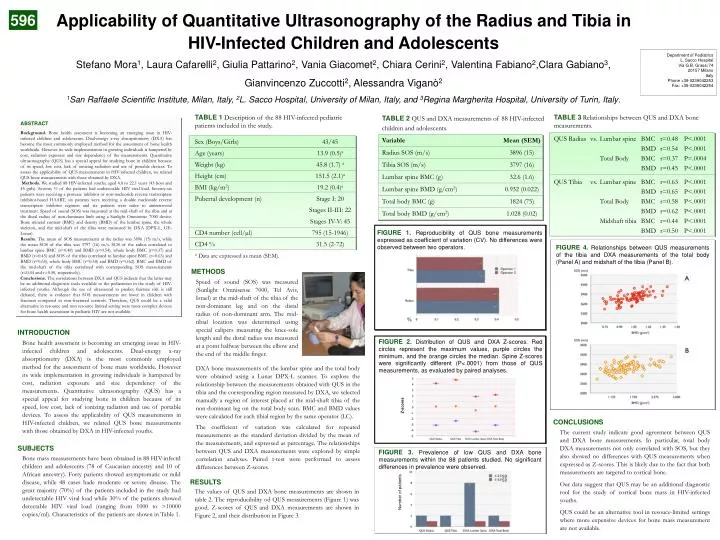
TABLE 1 Description of the 88 HIV-infected pediatric patients included in the study. Sex (Boys/Girls) 43/45 Age (years) 13.9 (0.5)a Weight (kg) 45.8 (1.7) a Height (cm) 151.5 (2.1)a BMI (kg/m2) 19.2 (0.4)a Pubertal development (n) Stage I: 20 Stages II-III: 22 Stages IV-V: 45 CD4 number (cell/µl) 795 (15-1946) CD4 % 31.5 (2-72) aData are expressed as mean (SEM). TABLE 2 QUS and DXA measurements of 88 HIV-infected children and adolescents. Variable Mean (SEM) Radius SOS (m/s) 3896 (15) Tibia SOS (m/s) 3797 (16) Lumbar spine BMC (g) 32.6 (1.6) Lumbar spine BMD (g/cm2) 0.932 (0.022) Total body BMC (g) 1824 (75) Total body BMD (g/cm2) 1.028 (0.02) TABLE 3Relationships between QUS and DXA bone measurements. QUS Radius vs. Lumbar spine BMC r=0.48 P<.0001 BMD r=0.54 P<.0001 Total Body BMC r=0.37 P=.0004 BMD r=0.45 P<.0001 QUS Tibia vs. Lumbar spine BMC r=0.63 P<.0001 BMD r=0.65 P<.0001 Total Body BMC r=0.58 P<.0001 BMD r=0.62 P<.0001 Midshaft tibia BMC r=0.44 P<.0001 BMD r=0.50 P<.0001 FIGURE 1.Reproducibility of QUS bone measurements expressed as coefficient of variation (CV). No differences were observed between two operators. FIGURE 4. Relationships between QUS measurements of the tibia and DXA measurements of the total body (Panel A) and midshaft of the tibia (Panel B). % FIGURE 2.Distribution of QUS and DXA Z-scores. Red circles represent the maximum values, purple circles the minimum, and the orange circles the median. Spine Z-scores were significantly different (P<.0001) from those of QUS measurements, as evaluated by paired analyses. Z-scores FIGURE 3.Prevalence of low QUS and DXA bone measurements within the 88 patients studied. No significant differences in prevalence were observed. SD SD Number of patients Applicability of Quantitative Ultrasonography of the Radius and Tibia in HIV-Infected Children and Adolescents Stefano Mora1, Laura Cafarelli2, Giulia Pattarino2, Vania Giacomet2, Chiara Cerini2, Valentina Fabiano2,Clara Gabiano3, Gianvincenzo Zuccotti2, Alessandra Viganò2 1San Raffaele Scientific Institute, Milan, Italy, 2L. Sacco Hospital, University of Milan, Italy, and 3Regina Margherita Hospital, University of Turin, Italy. 596 Department of Pediatrics L. Sacco Hospital Via G.B. Grassi 74 20157 Milano Italy Phone +39-0239042253 Fax: +39-0239042254 ABSTRACT Background. Bone health assesment is becoming an emerging issue in HIV-infected children and adolescents. Dual-energy x-ray absorptiometry (DXA) has become the most commonly employed method for the assessment of bone health worldwide. However its wide implementation in growing individuals is hampered by cost, radiation exposure and size dependency of the measurements. Quantitative ultrasonography (QUS) has a special appeal for studying bone in children because of its speed, low cost, lack of ionizing radiation and use of portable devices. To assess the applicability of QUS measurements in HIV-infected children, we related QUS bone measurements with those obtained by DXA. Methods. We studied 88 HIV-infected youths, aged 4.8 to 22.1 years (43 boys and 45 girls). Seventy % of the patients had undetectable HIV viral load. Seventy-six patients were receiving a protease inhibitor or non-nucleoside reverse transcriptase inhibitor-based HAART, six patients were receiving a double nucleoside reverse transcriptase inhibitor regimen and six patients were naïve to antiretroviral treatment. Speed of sound (SOS) was measured at the mid-shaft of the tibia and at the distal radius of non-dominant limb using a Sunlight Omnisense 7000 device. Bone mineral content (BMC) and density (BMD) of the lumbar spine, the whole skeleton, and the mid-shaft of the tibia were measured by DXA (DPX-L, GE-Lunar). Results. The mean of SOS measurements at the radius was 3896 (15) m/s, while the mean SOS of the tibia was 3797 (16) m/s. SOS of the radius correlated to lumbar spine BMC (r=0.48) and BMD (r=0.54), whole body BMC (r=0.37) and BMD (r=0.45) and SOS of the tibia correlated to lumbar spine BMC (r=0.63) and BMD (r=0.65), whole body BMC (r=0.58) and BMD (r=0.62). BMC and BMD of the mid-shaft of the tibia correlated with corresponding SOS measurements (r=0.44 and r=0.50, respectively). Conclusions. The correlations between DXA and QUS indicate that the latter may be an additional diagnostic tools available to the pediatrician in the study of HIV-infected youths. Although the use of ultrasound to predict fracture risk is still debated, there is evidence that SOS measurements are lower in children with fractures compared to non-fractured controls. Therefore, QUS could be a valid alternative in resource and non resource limited setting were more complex devices for bone health assessment in pediatric HIV are not available. METHODS Speed of sound (SOS) was measured (Sunlight Omnisense 7000, Tel Aviv, Israel) at the mid-shaft of the tibia of the non-dominant leg and on the distal radius of non-dominant arm. The mid-tibial location was determined using special calipers measuring the knee-sole length and the distal radius was measured at a point halfway between the elbow and the end of the middle finger. INTRODUCTION Bone health assesment is becoming an emerging issue in HIV-infected children and adolescents. Dual-energy x-ray absorptiometry (DXA) is the most commonly employed method for the assessment of bone mass worldwide. However its wide implementation in growing individuals is hampered by cost, radiation exposure and size dependency of the measurements. Quantitative ultrasonography (QUS) has a special appeal for studying bone in children because of its speed, low cost, lack of ionizing radiation and use of portable devices. To assess the applicability of QUS measurements in HIV-infected children, we related QUS bone measurements with those obtained by DXA in HIV-infected youths. DXA bone measurements of the lumbar spine and the total body were obtained using a Lunar DPX-L scanner. To explore the relationship between the measurements obtained with QUS in the tibia and the corresponding region measured by DXA, we selected manually a region of interest placed at the mid-shaft tibia of the non-dominant leg on the total body scan. BMC and BMD values were calculated for each tibial region by the same operator (LC). CONCLUSIONS The coefficient of variation was calculated for repeated measurements as the standard deviation divided by the mean of the measurements, and expressed as percentage. The relationships between QUS and DXA measurements were explored by simple correlation analyses. Paired t-test were performed to assess differences between Z-scores. The current study indicate good agreement between QUS and DXA bone measurements. In particular, total body DXA measurements not only correlated with SOS, but they also showed no differences with QUS measurements when expressed as Z-scores. This is likely due to the fact that both measurements are targeted to cortical bone. Our data suggest that QUS may be an additional diagnostic tool for the study of cortical bone mass in HIV-infected youths. QUS could be an alternative tool in resouce-limited settings where more expensive devices for bone mass measurement are not available. SUBJECTS Bone mass measurements have been obtained in 88 HIV-infectd children and adolescents (78 of Caucasian ancestry and 10 of African ancestry). Forty patients showed asymptomatic or mild disease, while 48 cases hade moderate or severe disease. The great majority (70%) of the patients included in the study had undetectable HIV viral load while 30% of the patients showed detectable HIV viral load (ranging from 1000 to >10000 copies/ml). Characteristics of the patients are shown in Table 1. RESULTS The values of QUS and DXA bone measurements are shown in table 2. The reproducibility od QUS measurements (Figure 1) was good. Z-scores of QUS and DXA measurements are shown in Figure 2, and their distribution in Figure 3.