Download
1 / 46
490 likes | 866 Vues
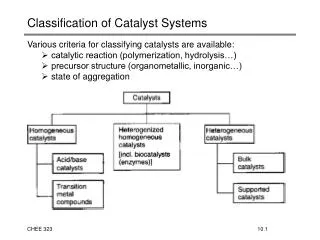
Diagnostic versus Classification Criteria: a continuum. Hasan Yazıcı University of Istanbul. 1. I have no conflicts of interest. Plan & Summary. Pre-test disease odds. Diagnosis. Classification. Ottawa Ankle Rules. IG Stiell et al. Ann Emerg Med 1992 .

E N D
Diagnostic versusClassification Criteria:a continuum Hasan Yazıcı University of Istanbul 1
Plan & Summary Pre-test disease odds Diagnosis Classification
Ottawa Ankle Rules IG Stiell et al. Ann Emerg Med 1992
EULAR/ACR Vasculitis Criteria Group (2008) “Perhaps the most robust criteria pertain to Behçet’s disease, where international collaboration has led to a validated proposal effective for both clinical and research purposes.” “The challenge of producing validated diagnostic criteria for these heterogeneous diseases that are suitable for use in clinical research as a classification tool, is a formidable one. However, as the international community has exemplified with Behçet’s disease, it is achievable.” 6
International Study Group Diagnostic Criteria (Lancet, 1990) Oral ulcers (~100%) + Two of below: Genital ulcers (80%) Skin lesions (80%) Eye lesions (50 %) Pathergy (50 %) Classification 7
Methods • 914 unselected (366 from Iran..... 9 from France) patients with BS from 12 centers in 7 countries • 28 BS patients without OU excluded • Control group: 308 patients with connective tissue diseases, including 97 with OU only • Study questionnaire based on previously published BS criteria sets • Individual disease features of a random sample (60%) were compared with those in the control group. Sensitivities, specificities, log likelihood ratios and expected weights of evidence were calculated for each symptom or sign. • Features were added to the criteria set up to the point at which there was no further contribution to the criteria by the expected weight of evidence of a particular disease feature. • The new criteria set were further validated in the 40% sample.
Turing’s expected weight of evidence • It is the sum of the individual weights of evidence (logeLR). • It represents the weight of a question while the answers make up individual weights of evidence. DJ Spiegelhalter Clin Gastroenterol 1985
Issuesapart from the – by definition- circular nature of the exercise • The initial internal validation was, in fact, an internal check of the initial randomization. • The questionnaire did not seek for the frequency of various features of diseases that made up the control group, among the BS patients. • All work and validations were retrospective. • No attempt at confidence intervals.
ACR Vasculitis Criteria*CHCC Vasculitis Criteria ** • Among 198 patients (51 with vasculitis) the positive predictive value of ACR criteria ranged 17% - 29% (JK Rao et al Ann Int Med 1998) • CHCC criteria correctly identifed 8/27 patients with Wegener’s and 4/12 with MPA (SF Sorensen et al Ann Rheum Dis 2000) 19
Hunder GG. The Use and Misuse of Classification and Diagnostic Criteria for Complex Diseases. Ann Intern Med 1998 20
ACR Classification criteria • RA • SLE • Sjogren • Vasculitis • Fibromyalgia • JRA • Osteoarthritis • Scleroderma
The“circular” logic in diagnostic/classification criteria for conditions which lack a specific laboratory or a histological feature JF Fries Arch Intern Med 1984 A perpetual motion machine, 1660 Wikipedia
Pre-test disease odds Diagnosis Classification
Bayes theorem in c/d post-test odds = pre-test odds x LR LR = likelihood ratio 24
Bayes theorem in c/d post-test odds = pre-test odds x LR LR = likelihood ratio 25
Bayes theorem in c/dPre-test odds post-test odds = pre-test odds x LR actual disease prevalance (when c/d) or frequency of disease manifestations in the disease studied vs. in diseases that come into the differential diagnosis(when formulating LR’s) 26
Bayes theorem in c/d post-test odds = pre-test odds x LR LR = likelihood ratio 27
Bayes theorem in c/d post-test odds = pre-test odds x LR c/d criteria LR = likelihood ratio 28
Bayes theorem in c/dLikelihood ratio (LR) post-test odds = pre-test odds x LR + LR = sensitivity/1-specificity or % true positives/% false positives - LR = 1-sensitivity or % true negatives/% false negatives 29
The Circular Nature • We use elements of pre-test odds (es) to estimate the LR’s. • From these LR’s we estimate the classification LR (criteria). • We use another (but related!) pre-test odds to estimate the post-test odds (c/d).
Fulfilling the ISBD Criteria: What does it mean? (sensitivity = 90%; specificity =95%) Criteria + (+LR) : 0.90/1-0.95 = 18 x pre-test odds Criteria - (-LR) : 1 - 0.90 /0.95 = 0.10 x pre-test odds 31
Sensitivity = 0.95 (0.90)Specificity = 0.95 • + LR Sensitivity/1-Specificity = 19 (18) • - LR 1- Sensitivity/Specificity = 0.05 (10)
Sensitivity = 0.90Specificity = 0.97 (0.95) • + LR Sensitivity/1-Specificity = 30 (18) • - LR 1- Sensitivity/Specificity = 0.10 (10)
Specificity constant Increasing sensitivity Sensitivity constant Increasing specificity 34
“Diagnostic criteria apply to individual persons rather than groups. In order to establish a correct diagnosis and to ensure that cases are not missed, such criteria should have a high sensitivity (especially for early cases of a particular disease, e.g. early ankylosing spondylitis) and will often include items that are present already early in the disease course. Such an approach will reduce specificity, which means that more false positives might be expected. Diagnostic criteria are mainly applied in clinical practice, an environment in which, at least for a limited follow-up period, a false-positive diagnosis is considered more acceptable than a false-negative rejection of a diagnosis.” Rheumatology 4 Ed. 2008
Classification For groups High specificity Diagnosis For individuals High sensitivity Classification vs. DiagnosticCriteria??? Rheumatology 4 Ed. 2008
“With this adaptation the sensitivity increased from 76% for the original New York criteria to 83% for the modified New York criteria, whereas the specificity only decreased from 99% to 98%.” Rheumatology 4 Ed. 2008
Original NY criteria Sensitivity: 76% Specificity: 99% + LR: 0.76/1-0.99 = 76 (3.2:1) - LR: 1-0.76/0.99 = 0.24 (500:1) Modified NY criteria Sensitivity: 83% Specificity: 98% + LR: 0.83/1-0.98 = 42 (0.7:1) - LR: 1-0.83/0.98 = 0.17 (588:1) LR’s and Odds of disease(assuming 1/100 frequency of AS)
What to do? • Define well your pre-test odds. • Go to well defined practices (subspecialties).
Causes of Uveitis (%) in Japan* & USA** * H Goto et al. Jpn J Ophtalmol 2007; ** A Rodriquez et al. Arch Ophthalmol1996
Conclusions • There are no separate classification or diagnostic criteria but c/d criteria. • Classification and diagnosis are components of a continuum of which epidemiology is a most integral part. • To make a diagnosis is not an art but science backed by experience and arithmetic.
A Proposal • Avoid attempts for “universal” disease criteria and • Aim for classification/diagnostic criteria for subspecialties 44 H Yazici et al. Arthritis Rheum, 2008
Proposed Scheme of Preparing c/d Criteria in a Subspecialty Setting • Retrospective tabulation of demography and diagnoses (old & new pts.; 6 mo.) • Same on new patients with checklists (crossed) of symptoms/findings /lab./rad./hist. (6 mo.) • Estimation of clinical prediction rules and classification criteria after selecting the comparator groups • Internal and external validation of the criteria in the same and different settings (new patients; 6 mo.)
Confidence Intervals • 9/10 = 900/1000 • MC Reid, MS Lachs, AR Feinstein JAMA 1995 • 9/10 ≠ 900/1000