Download
1 / 78
860 likes | 1.49k Vues
Antiphospholipid Antibody Syndrome. Thomas L. Ortel, M.D., Ph.D. Duke Hemostasis & Thrombosis Center 30 September 2006. Patient History. 59 yr old man admitted locally with chest pain, found to have a non-Q-wave MI.

E N D
Antiphospholipid Antibody Syndrome Thomas L. Ortel, M.D., Ph.D. Duke Hemostasis & Thrombosis Center 30 September 2006
Patient History • 59 yr old man admitted locally with chest pain, found to have a non-Q-wave MI. • Remote history of DVT and PE, on chronic oral anticoagulant therapy (target INR?). • Warfarin discontinued, and cardiac catheterization performed.
Patient History • Complex LAD stenosis treated by angioplasty and stent placement. • Recurrent chest pain during same admission. Repeat catheterization found thrombus in stent. LAD and 1st diagonal branch restented. • Recurrent chest pain one week later resulted in 2-vessel CABG.
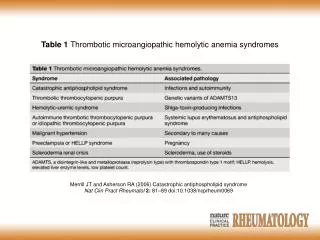
Patient History • Re-admit one week later with fever, new CHF, and elevated liver function enzymes. • Echocardiogram revealed ‘severe cardiomyopathy’. • CT scan revealed multiple liver lesions, felt to be either ‘cysts or abscesses’. • Transfer to Duke because of ‘coagulopathy’ and need to biopsy…
Antiphospholipid Syndrome A clinicopathologic diagnosis…
Sapporo Criteria (Updated) • International Consensus Statement on Classification Criteria for APS (2006). • Clinical criteria. • Vascular thrombosis. • Pregnancy morbidity. • Laboratory criteria. • Lupus anticoagulant. • Anticardiolipin IgG or IgM antibody. • Anti-b2glycoprotein I IgG or IgM antibody. -- Miyakis, et al., J.Thromb.Haemost., 2006; 4: 295-306.
Clinical criteria for APS • Vascular thrombosis*. • Venous thromboembolic disease (DVT, PE). • Arterial thromboembolic disease. • Small vessel thrombosis. * “Coexisting inherited or acquired thrombotic risk factors are not reasons for excluding patients from a diagnosis of APS trials.” -- Miyakis, et al., J.Thromb.Haemost., 2006; 4: 295-306.
Clinical criteria for APS • Pregnancy morbidity. • One or more unexplained deaths of a morphologically normal fetus at or beyond10th week of gestation. • Three or more unexplained spontaneous abortions at or prior to 10th week of gestation. • One or more premature births at or before the 34th week of gestation due to eclampsia or placental insufficiency. -- Miyakis, et al., J.Thromb.Haemost., 2006; 4: 295-306.
Laboratory criteria for APS • Lupus anticoagulant: defined by a functional, clot-based assay using the ISTH guidelines. • Anticardiolipin IgG or IgM antibody. • Anti-b2glycoprotein I IgG or IgM antibody. --Measured on 2 or more occasions at least 12 weeks apart. -- Miyakis, et al., J.Thromb.Haemost., 2006; 4: 295-306.
ISTH criteria for lupus anticoagulants • Prolongation of a phospholipid-dependent screening assay; • Evidence of inhibitory activity; • Evidence that inhibitory activity is phospholipid-dependent; and, • Distinction from other ‘coagulopathies’…
“Non-criteria” APS findings • Thrombocytopenia and/or hemolytic anemia. • Transverse myelopathy or myelitis. • Livido reticularis. • Cardiac valve disease. • Nephropathy. • Non-thrombotic neurologic manifestations, including multiple sclerosis-like syndrome, chorea, or migraine headaches. -- Miyakis, et al., J.Thromb.Haemost., 2006; 4: 295-306.
Did our patient meet clinical criteria for APS? • Major criteria: • Deep venous thrombosis & pulmonary embolism. • Myocardial infarction and stent thrombosis (age < 60 yrs.). • Non-criteria APS-associated parameters: • Thrombocytopenia.
Did our patient meet clinical criteria for APS? • Major criteria: • Deep venous thrombosis & pulmonary embolism. • Myocardial infarction and stent thrombosis (age < 60 yrs.). • Non-criteria APS-associated parameters: • Thrombocytopenia. Yes.
Did our patient meet laboratory criteria for APS? • Initial assessment: • Prolonged PT and aPTT that did not correct with mixing studies. • Decreased factor VIII, IX, and XI levels. • A detectable factor VIII inhibitor by Bethesda assay. • Prolonged DRVVT but could not complete the CONFIRM portion of the assay.
Did our patient meet laboratory criteria for APS? • Initial assessment: • Prolonged PT and aPTT that did not correct with mixing studies. • Decreased factor VIII, IX, and XI levels. • A detectable factor VIII inhibitor by Bethesda assay. • Prolonged DRVVT but could not complete the CONFIRM portion of the assay. No... but…
Alternative strategies to identify a lupus anticoagulant • Platelet neutralization procedure (PNP; uses platelet membranes). • Hexagonal phase phospholipid assay (StaClot LA; uses PE in a hexagonal phase conformation). • Textarin/Ecarin clot time. • Factor V analysis by PT and aPTT-based assays.
Assessment ofCoagulation Tests • Lupus anticoagulant detected and confirmed. • Multiple factor deficiencies in aPTT pathway reflect high-titer lupus anticoagulant. • Prolonged PT reflects mild factor II deficiency and lupus anticoagulant effect. • Elevated D-dimer reflects recent thrombosis. • Elevated inhibitor titer due to lupus anticoagulant.
What are the clinical implications of an elevated antiphospholipid antibody level?
Frequency of antiphospholipid antibodies in different populations
Risk of thrombosis in patients with antiphospholipid antibodies • Incidence of thrombosis: ~2-2.5%†. • Coincident risk factors for thrombosis: up to 50%‡. • Lupus (1997) 6: 467. ** Lupus (1998) 7: 15. • † Am J Med (1996) 100: 530. ‡ J Rheumatol (2004) 31: 1560.
Antiphospholipid antibodies in patients with venous thromboembolism * LAC only. † Anticardiolipin & LAC. ‡ Anticardiolipin only.
Do any of the clinical laboratory tests identify patients at risk for thromboembolic problems?
Lupus anticoagulants, anticardiolipin antibodies, and thrombosis -- Galli, et al., Blood, 2003; 101: 1827.
Anticardiolipin antibody titerand thrombosis -- Galli, et al., Blood, 2003; 101: 1827.
What is the optimal antithrombotic therapy for a patient with APS and thromboembolism?
Target INR in patients with APS and venous thrombosis • Retrospective studies. • Prospective studies investigating oral anticoagulant therapy that included patients subsequently found to have antiphospholipid antibodies. • Prospective randomized clinical trials.
Target INR in patients with APS and venous thrombosis • Retrospective studies. • Rosove & Brewer (1992): 70 patients with APS and thrombosis. No thrombosis when INR ≥ 3.0. • Khamashta, et al. (1995): 147 patients with APS and thrombosis. Of 42 recurrent events on warfarin, 3 occurred with an INR ≥ 3, compared to 39 with INR < 3.
Recurrent Thrombosis in APS Warfarin, INR ≥ 3.0 Warfarin, INR < 3.0 ASA None -- Khamashta, et al., N Eng J Med, 1995; 332: 993.
Caveats about theretrospective studies • Retrospective study design. • Heterogenous management of anticoagulant therapy. • Many patients had secondary APS. • Most of the patients had recurrent thrombosis. • Hemorrhagic complications relatively common.
Target INR in patients with APS and venous thrombosis • Prospective studies. • Schulman, et al. (1998): 412 patients with a first episode of venous thromboembolism treated for 6 months with oral anticoagulants with a target INR of 2.0 to 2.85. 68 patients (16.5%) had an anticardiolipin antibody detected at the time anticoagulation was stopped.
Target INR in patients with APS and venous thrombosis • Prospective randomized trials. • Crowther, et al. (2003): 114 patients with APS and thrombosis. Higher target INR (3.1 to 4) was not superior to standard target INR (2 to 3). • Finazzi, et al. (2005): 109 patients with APS and thrombosis. Higher target INR (3 to 4.5) was not superior to standard target INR (2 to 3).
Recurrent Thrombosis -- Crowther, et al., N Eng J Med, 2003; 349: 1133.
Caveats about theprospective randomized trials • Patients with previous thrombotic recurrence were excluded. • Few patients with secondary APS. • Few patients with arterial thromboembolism. • Patients in the high-intensity group more frequently ‘subtherapeutic’ than those in the standard intensity group.
ACCP Guidelines • Treatment of venous thromboembolism in patients with antiphospholipid antibodies. • We recommend … a target INR of 2.5 (INR range, 2.0 and 3.0) (Grade 1A). We recommend against high-intensity VKA therapy (Grade 1A). -- Buller, et al., Chest, 2004; 126 (Supplement): 401S.
How long should patients with APS and venous thrombosis be treated with warfarin? • Schulman, et al., 1998. • Prospective study. • 412 patients with 1st episode of venous thrombo-embolism treated for 6 months with warfarin. • 68 patients (17%) with elevated antibody levels when warfarin therapy stopped.
Anticardiolipin Antibodies and Recurrent Venous Thromboembolism -- Schulman, et al., Am J Med, 1998; 104: 332.
ACCP Guidelines • Treatment of venous thromboembolism in patients with antiphospholipid antibodies. • We recommend … a target INR of 2.5 (INR range, 2.0 and 3.0) (Grade 1A). We recommend against high-intensity VKA therapy (Grade 1A). • We recommend treatment for 12 months (Grade 1C+). • We suggest indefinite anticoagulant therapy for these patients (Grade 2C). -- Buller, et al., Chest, 2004; 126 (Supplement): 401S.
British Society of Haematology Guidelines • For patients with APS and venous thrombosis, treatment for 6 months with a target INR of 2.5 is reasonable. • Recurrent venous thrombosis should be treated by “long-term” oral anticoagulation. • Recurrence while the INR is between 2.0 and 3.0 should lead to more intensive warfarin therapy, target INR 3.5, but this is “uncommon”. -- Greaves, et al., Br.J.Haematol., 2000; 109: 704-15.
How do I treat venous thromboembolism in APS? • Confirm baseline PT is normal. • For an initial event, oral anticoagulation with a target INR of 2.5 for 12 months. Consider longer pending clinical course. • Address additional prothrombotic risk factors. • For recurrent events, consider more aggressive or alternative anticoagulation, or other strategy.
What about patients with APS and arterial thromboembolism? • Retrospective studies suggest target INR > 3.0. • Rosove & Brewer (1992). • Khamashta, et al. (1995). • Prospective randomized trials suggest target INR of 2 to 3. • Crowther, et al. (2003). • Finazzi, et al. (2005).
Antiphospholipid Antibodies and Recurrent Stroke • The APASS Investigators, 2004. • Prospective cohort study. • Conducted within the WARSS study. • Compared warfarin (target INR 1.4 to 2.8) vs. ASA. • Analyzed antiphospholipid status after stroke. • Composite outcome measure including death, ischemic stroke, or other thromboembolic events.
APASS Study Outcomes -- APASS Investigators, JAMA, 2004; 291: 576.
Caveats about the APASS study • Patients were stratified according to a single determination of anticardiolipin antibody status. • Patients in this study were older than most patients with APS. • Target INR was lower than what is frequently used to prevent recurrent thromboembolic events.
What about antiplatelet therapy alone in patients with APS and stroke/TIA?
Aspirin for APS with ischemic stroke • Eight patients with ischemic stroke as the initial thrombotic presentation of APS. • All were women, mean age of 35.5 years (range, 26-47 years). • Two patients sustained a recurrent stroke during 8.9 years of follow-up (recurrence rate of 3.5 per 100 patient-years). One sustained a DVT. -- Derksen, et al., Neurology, 2003; 61: 111-4.
ACCP Guidelines • Prevention of noncardioembolic cerebral ischemic events. • For most patients, we recommend antiplatelet agents over oral anticoagulation (Grade 1A). • For patients with ‘well-documented’ prothrombotic disorders, we suggest oral anticoagulation over antiplatelet agents (Grade 2C). -- Albers, et al., Chest, 2004; 126 (Supplement): 483S.
British Society of Haematology Guidelines • Because of the high risk of recurrence and likelihood of consequent permanent disability or death, stroke due to cerebral infarction in APS should be treated with long-term oral anticoagulant therapy, target INR 2.5 (optimal range 2.0-3.0) (level III evidence, grade B recommendation). -- Greaves, et al., Br.J.Haematol., 2000; 109: 704-15.