Download
1 / 40
410 likes | 947 Vues
SQUAMOUS CELL CARCINOMA OF THE ESOPHAGUS . GENERAL THORACIC SURGERY CHAPTER 143. ETIOLOGY. No specific etiology agent. Poverty and malnutrition. High dietary content of nitrosamines, nitrites. Tobacco, betel nut, chronic esophageal irritation. Lye burn.

E N D
SQUAMOUS CELL CARCINOMA OF THE ESOPHAGUS GENERAL THORACIC SURGERY CHAPTER 143
ETIOLOGY • No specific etiology agent. • Poverty and malnutrition. • High dietary content of nitrosamines, nitrites. • Tobacco, betel nut, chronic esophageal irritation. • Lye burn. • Achalasia, peptic reflux esophagitis.
Pathology • Rare below age 30. • Common located in middle-third(carina to inferior pulmonary vein). • Microscopic feature— Early-stage esophageal cancer—intraepitherlial, intramucosal, submucosal carcinoma. No lymph node metastases.
Molecular biology • p53 gene mutation in invasive lesion. • Over expression of HER2/new. • Amplification of cyclin D gene. • Frequent mutation p16 multiple suppressor cyclin-dependent kinase 4 inhibitor gene.
Metastases • Direct extension. • Lymphatic metastases (60%). • Hematogenous metastases(50-63%). • Distal metastases — 25-30% at time of diagnosis.
Metastases • Intraesophageal spread—microscopic spread is greater than macroscopic spread. • Submucosal lymphatic spread occurs often, may result in tumor emboli producing skip or satellite nodules.
Metastases • Direct extension—tumor penetrating adventitial layer. • Upper third invasion to mediastinum, great vessel, trachea, recurrent laryngeal nerve. • Middle third invasion to pleura, left main bronchus, aorta, pericardium. • Lower third invasion to diaphragm stomach.
Metastases • Lymphatic spread—the direction of esophageal lymph flow is longitudinal, cephalad or caudad. • Upper third tend to be cephalad. • Lower two third is caudad, incidence 40-60%. • Related to depth and extent of invasion.
Lymph node station • 1 — the paraesophageal lymph node. • 2 — periesophageal, celiac perigastric lymph node. • 3 — the distal subdiapgragm or supraclavicular, lateral thoracic region.
Clinical manifestation • s/s — infrequently at early stage. • Retrosternal discomfort, pain sensatin of frication, burning. • Slow passage of food during swallowing. • Progressive dysphagia — first solid food, then soft food, then liquid. • Melena, hematemess, anemia, weight loss, hoarseness, hiccough, cachexia.
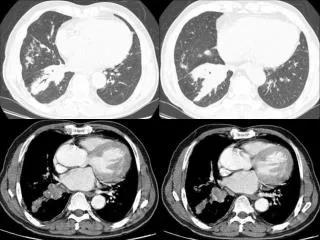
Diagnostic studies • Cytologic screening • Upper GI series • CT • Endoscopy • Endoscopic ultrasonography • Bronchoscopy: evaluation the tracheal or bronchial invasion.
Cytologic screening • Screen asymptomatic people in high-incidence area. • Obtain smear of esophageal mucosa with abrasive balloon catheter.
Upper GI series • Diffucult in demonstration the early lesion • Length of lesion, not correlate with degree of tumor penetration. • Longer than 10 cm is incurable. • Esophageal axis, 74% tumor penetrated wall associated with axis abnormalities. • Demonstration tracheoesophageal fistula.
CT • Four stage — I — intralumonal mass without wall thickening. II — wall thickening. III — tumor spread into adjacent tissue. IV — distal meatastases. • Identified lymph node. • Aortic invasion: loss fat planes and contact less hen 45 degree — invasion unlikely; exceed 90 degree — invasion real possibility. • Invasion to pericardium is difficult to detect.
Endoscopy • Essential in all patients. • Biopsy should be done in all cases. • Positive diagnosis 90%. • If no lesion—mucosal stain— Toluidine blue stain — the tumor cell not the normal nucosa. Lugol’s solution stain — the normal cell not the tumor cell.
Endoscopic ultrasonography • —detailed studies the structure of esophageal wall and periesophageal tissue.
Staging • —TNM system.
Surgical therapy • Transthoracic, trandhiatal esophagectomy. • Reconstruction. • Respectability rate—45%-56%. • Morbidity—most respiratory complication. • Mortality—0.8%-12%. • Surgical result—long-term survival is poor.
Resection plus adjuvant therapy • Preoperative radiation therapy • Postoperative irradiation
Preoperative radiation therapy • Tumor became smaller and softer. • Less infiltrating tissue plane develop. • Increase respectability. • Long term survival unchanged.
Postoperative irradiation • No survival advantage. • Significant reduction in local recurrence. • High incidence of complication related the transposed intrathoracic stomach.
Chemotherapy • Response rate — 40-60%. • Neoadjuvant chemotherapy.
Fate of surgically resected patient • Survive more than 5 year tend to have the follow prognostic factors— Small tumor less than 5 cm long. No invasion to advantia. No lymph node involvement. Age younger than 60 year. Women.