Download
1 / 86
870 likes | 1.1k Vues
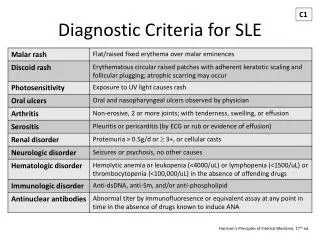
SLE. HLA class I, class II , and class III are associated with SLE, but only classes I and II contribute independently to increased risk of SLE

E N D
SLE • HLA class I, class II, and class III are associated with SLE, but only classes I and II contribute independently to increased risk of SLE • Other genes which contain risk variants for SLE are IRF5, PTPN22, STAT4, CDKN1A, ITGAM, BLK, TNFSF4 and BANK1. Some of the susceptibility genes may be population specific
screening • Firstly, there is screening of individuals and couples known to be at significant or high risk because of a positive family history-sometimes referred to as targeted, or family, screening because it focuses on those most likely to benefit. This includes carrier, or heterozygote, screening, as well as presymptomatic testing. • Secondly, there is the screening offered to the general population, who are at low risk-this is sometimes referred to as community genetics.
Screening • Population screening involves the offer of genetic testing on an equitable basis to all relevant individuals in a defined population. • Its primary objective is to enhance autonomy by enabling individuals to be better informed about genetic risks and reproductive options. • A secondary goal is the prevention of morbidity due to genetic disease and alleviation of the suffering that this would impose.
SCREENING THOSE AT HIGH RISK • If it was easy to recognize carriers of autosomal and X-linked recessive disorders and persons who are heterozygous for autosomal dominant disorders which show reduced penetranceor a late age of onset, much doubt and uncertainty would be removed when providing information in genetic counseling.
CARRIER TESTING FOR AUTOSOMAL RECESSIVE AND X-LINKED DISORDERS • In a number of autosomal recessive disorders, such as some of the inborn errors of metabolism, e.g. Tay-Sachs disease, and the hemoglobinopathies, e.g. sickle-cell disease, carriers can be recognized with a high degree of certainty using biochemical or hematological techniques such that DNA analysis is not necessary. • In other single-gene disorders, it is possible to detect or confirm carrier status by biochemical means in only a proportion of carriers, e.g. the presence of abnormal coagulation studies in a woman at risk of being a carrier for hemophilia. • A significant proportion of obligate carriers of hemophilia will have normal coagulation, however, so that a normal result in a woman at risk does not exclude her from being a carrier.
Occasionally, carriers for certain disorders can have mild clinical manifestations of the disease
BIOCHEMICAL ABNORMALITIES IN CARRIERS • In some disorders the biochemical abnormality seen is a direct product of the gene and the carrier status can be tested for with confidence. For example, in carriers of Tay-Sachs disease the range of enzyme activity (hexosaminidase) is intermediate between levels found in normal and affected persons. • In many inborn errors of metabolism, however, the enzyme activity levels in carriers overlap with the normal range, so that it is not possible to reliably distinguish between heterozygote carriers and those who are homozygous normal.
Indirect • A grossly elevated serum creatinekinase (CK) often confirms the diagnosis of DMD in a boy presenting with features of the disorder. • Obligate female carriers of DMD have, on average, serum CK levels that are elevated compared to those of the general female population. There is, however, a substantial overlap of CK values between normal and obligate carrier females.
Random inactivation of the X chromosome • There is another reason for difficulty with carrier testing in the case of X-linked recessive disorders. Random inactivation of the X chromosome in females means that many, often the majority, of female carriers of X-linked disorders cannot be reliably detected by biochemical methods.
PRESYMPTOMATIC DIAGNOSIS OF AUTOSOMAL DOMINANT DISORDERS • Many autosomal dominant single-gene disorders either have a delayed age of onset or exhibit reduced penetrance. • The results of clinical examination, specialist investigations, biochemical studies and family DNA studies can allow one to predict whether a person has inherited the gene before the onset of symptoms or signs. This is known as presymptomatic diagnosis or predictive testing
CLINICAL EXAMINATION • It is not unusual to examine an apparently unaffected relative of someone with NF1 who has had no medical problems, only to discover that they have sufficient numbers of a diagnostic feature, such as café-au-lait spots or cutaneousneurofibromas, to confirm that they are affected. However, NF1 is a relatively rare example of a dominantly inherited disorder that is virtually 100% penetrant by the age of 5 or 6 years, with visible external features. With many other disorders clinical examination presents greater challenges. • Reaching a diagnosis in Marfansyndrome can be notoriously difficult because of the variable features and the overlap with other joint hypermobility disorders, even though very detailed diagnostic criteria have been established. • Poly cystic kidney • Tuberous sclerosis
In TSC imaging studies of the brain by CT scan to look for intracranial calcification is a more or less routine investigation, as well renal ultrasound to identify the cysts known as angiomyolipoma(ta). Use of these relatively non-invasive tests in relatives of persons with TSC can detect evidence of the condition in asymptomatic persons.
SPECIALIST INVESTIGATION (Intracranial calcification (arrowed) in an asymptomatic person with tuberous sclerosis
It is important to point out, however, that the absence of these findings on clinical or specialist investigation does not always exclude the diagnosis of the disorder being tested for but does reduce the likelihood of the person concerned having inherited the gene.
BIOCHEMICAL TESTS • In a number of autosomal dominant disorders biochemical tests can determine whether or not a person at risk has inherited a gene. Examples include the use of serum cholesterol levels in persons at risk for familial hypercholesterolemia and assay of the appropriate urinary porphyrinsor the specific enzyme deficiency in the various dominant porphyrias
Autosomal disorders that show a delayed age of onset or exhibit reduced penetrance in which linked DNA markers or specific mutational analysis can be used to offer presymptomatic diagnosis
Familial adenomatouspolyposis • in persons at risk for familial adenomatouspolyposis, colonoscopy looking for the presence of colonic polyps can be offered as a regular screening procedure to those who have been shown to be at high risk of developing colonic cancer by molecular studies. Conversely, individuals who have been shown not to have inherited a mutation in the APC gene do not need to be screened.
In contrast, for persons at risk for HD, in which there is not yet any effective treatment to delay the onset or progression of the disorder, the benefit of predictive testing is not immediately obvious. • It is possible that employers, life insurance companies and society in general will put indirect and, on occasion, direct pressure on persons at risk for inherited disorders to have such testing.
Sensitivity: a / (a + c)-proportion of true positives; specificity: d / (d + b)-proportion of true negatives
Sensitivity: 96 / (96 + 4) = 96%; specificity is 510 100 / (510 100 + 4980) = ∼99%
Table 20.5 explains this further. Of great interest too is the positive predictive valueof a screening test, which is the proportion of positive tests that are true positives, and this is illustrated in Table 20.6.
Newborn screening programs • Newborn screening programs have been introduced on a widespread basis for phenylketonuria, galactosemia and congenital hypothyroidism. • In all of these disorders early treatment can prevent the development of learning disabilities.
The case of newborn screening for Duchenne muscular dystrophy also deviates from the screening paradigm because there is no effective treatment. • In this situation the indication is to try to identify families for whom genetic counseling could be offered with a view to alerting relevant females to their possible carrier status.
PHENYLKETONURIA • Routine biochemical screening of newborn infants for phenylketonuria was recommended by the Ministry of Health in the UK in 1969 after it had been shown that a low-phenylalanine diet could prevent the severe learning disabilities that previously had been a hallmark of this condition • The screening test, which is sometimes known as the Guthrie test, is carried out on a small sample of blood obtained by heel-prick at age 7 days. • An abnormal test result is further investigated by repeat analysis of phenylalanine levels in a venous blood sample. A low-phenylalanine diet is extremely effective in preventing learning
Newborn screening programs • . Any woman with phenylketonuria who is contemplating pregnancy should adhere to a strict low-phenylalanine diet both before and during pregnancy to minimize the risk of brain damage to her unborn child
GALACTOSEMIA • Classic galactosemia affects approximately 1 in 50 000 newborn infants and usually presents with vomiting, lethargy and severe metabolic collapse within the first 2 or 3 weeks of life. • Newborn screening is based on a modification of the Guthrie test with subsequent confirmation by specific enzyme assay. The early introduction of appropriate dietary restriction can prevent the development of serious complications such as cataracts, liver failure and learning disabilities.
CONGENITAL HYPOTHYROIDISM • Screening for congenital hypothyroidism was first introduced in the USA in 1974 and is now undertaken in most parts of the developed world. • treatment with life-long thyroxine replacement is extremely effective in preventing the severe developmental problems associated with the classic picture of 'cretinism'. The most common cause of congenital hypothyroidism is absence of the thyroid gland rather than an inborn error of metabolism
CYSTIC FIBROSIS • It is based on the detection of an elevated blood level of immunoreactivetrypsin (IRT), which is a consequence of blockage of pancreatic ducts in utero, supplemented by DNA analysis • The rationale for screening is that it is hoped that early treatment with physiotherapy and antibiotics will improve the long-term prognosis.
SICKLE-CELL DISEASE AND THALASSEMIA • Newborn screening based on hemoglobin electrophoresis is undertaken in many countries with a significant Afro-Caribbean community. • . In the case of sickle-cell disease, treatment involves the use of oral penicillin to reduce the risk of pneumococcal infection resulting from immune deficiency secondary to splenic infarction
POPULATION CARRIER SCREENING • Widespread screening for carriers of autosomal recessive disorders in high-incidence populations was first introduced for the hemoglobinopathiesand has been extended to several other disorders. • The rationale behind these programs is that carrier detection can be supported by genetic counseling so that carrier couples can be forewarned of the 1 in 4 risk that each of their children could be affected.
POPULATION CARRIER SCREENING • In Cyprus in 1974 the birth incidence of β-thalassemia was 1 in 250 (carrier frequency 1 in 8). Following the introduction of a comprehensive screening program to determine the carrier status of young adults, which had the support of the Greek Orthodox Church, the incidence of affected babies declined by over 95% within 10 years • Similar programs in Greece and Italy have seen a drop in the incidence of affected homozygotes of over 50%.
Amniocentesis • Amniocentesis involves the aspiration of 10-20ml of amniotic fluid through the abdominal wall under ultrasound guidance • This is usually performed around the 16th week of gestation. The sample is spun down to yield a pellet of cells and supernatant fluid. • The fluid can be used in the prenatal diagnosis of neural tube defects by assay of α-fetoprotein • The availability of PCR has meant that direct DNA analysis is usually possible without the need for culture. • When a couple is considering amniocentesis as an option they should be informed of the 0.5-1% risk of miscarriage associated with the procedure
CHORIONIC VILLUS SAMPLING • In contrast to amniocentesis, chorionic villus sampling (CVS), which was first developed in China, enables prenatal diagnosis to be undertaken during the first trimester. • This procedure is usually carried out at 11-12 weeks gestation under ultrasound guidance by either transcervical or, more usually, transabdominal aspiration of chorionic villi
Chromosome analysis can be undertaken on chorionic villieither directly, looking at metaphase spreads from actively dividing cells, or following culture. • Direct chromosomal analysis of chorionic villi usually allows a provisional result to be given within 24h.
CVS • although it has the disadvantage that even in experienced hands this procedure conveys a 1-2% risk of causing miscarriage. • There is also evidence that this technique can cause limb abnormalities in the embryo if carried out before 9-10 weeks gestation - for this reason CVS is not now performed before 11 weeks gestation.
ULTRASOUND • ULTRASOUND can be used not only for obstetric indications, such as placental localization and the diagnosis of multiple pregnancies, but also for the prenatal diagnosis of structural abnormalities that are not associated with known chromosomal, biochemical or molecular defects. • For example, a search can be made for polydactylyas a diagnostic feature of a multiple abnormality syndrome, such as one of the autosomal recessive short-limb polydactyly syndromes that are associated with severe pulmonary hypoplasia and are invariably lethal. Similarly,
however, detailed 'fetal anomaly' scanning is being offered routinely to all pregnant women at around 18 weeks gestation as a screening procedure for structural abnormalities such as neural tube defects or cardiac anomalies. • In addition, the observation that increased nuchal translucency (NT) is seen in fetuses who are subsequently born with Down syndrome, has resulted in the introduction of measurements of nuchal pad thickness in the first and second trimesters as a screening test for Down syndrome
FETOSCOPY • Fetoscopy involves visualization of the fetus by means of an endoscope. Increasingly, this technique is being superseded by detailed ultrasound scanning, although occasionally fetoscopy is still undertaken during the second trimester to try to detect the presence of subtle structural abnormalities that would point to a serious underlying diagnosis.
Fetoscopy has also been used to obtain samples of tissue from the fetus that can be analyzed as a means of achieving the prenatal diagnosis of several rare disorders like epidermolysisbullosa (skin) and ornithinetranscarbamylase deficiency (liver) • Unfortunately, fetoscopy is associated with a 3-5% risk of miscarriage.