Download
1 / 12
120 likes | 236 Vues
Liver and Pancreas Lab Work. Dr. Felix Hernandez M.D. Hepatic Function Tests. Are used to asses the health, function and stability of the liver. All hepatocytes contain these enzymes within them and they are released into circulation once the hepatocytes are damaged.

E N D
Liver and Pancreas Lab Work • Dr. Felix Hernandez M.D.
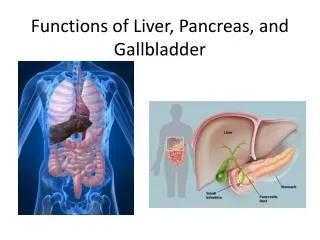
Hepatic Function Tests • Are used to asses the health, function and stability of the liver. • All hepatocytes contain these enzymes within them and they are released into circulation once the hepatocytes are damaged. • Includes Aspartate aminotransferase (AST), Alanine aminotransferase (ALT), Alkaline phosphatase, and Bilirubin
Aspartate aminotransferase (AST) • serum (AST, SGOT, GOT) • 0–35 IU/L • [0–0.58 mckat/L] • Physiologic Basis • Intracellular enzyme involved in amino acid metabolism. Present in large concentrations in liver, skeletal muscle, brain, red cells, and heart. Released into the bloodstream when tissue is damaged, especially in liver injury. • Interpretation • Increased in: Acute viral hepatitis (ALT > AST), biliary tract obstruction (cholangitis, choledocholithiasis), alcoholic hepatitis and cirrhosis (AST > ALT), liver abscess, metastatic or primary liver cancer; right heart failure, ischemia or hypoxia, injury to liver ("shock liver"), extensive trauma. Drugs that cause cholestasis or hepatotoxicity. • Decreased in: Pyridoxine (vitamin B6) deficiency. • AST/ALT ratio >1 suggests cirrhosis in patients with hepatitis C.
Alanine aminotransferase • serum (ALT, SGPT, GPT) • 0–35 U/L • [0–0.58 mckat/L] • Physiologic Basis: • Intracellular enzyme involved in amino acid metabolism. Present in large concentrations in liver, kidney; in smaller amounts, in skeletal muscle and heart. Released with tissue damage, particularly liver injury. • Interpretation • Increased in: Acute viral hepatitis (ALT > AST), biliary tract obstruction (cholangitis, choledocholithiasis), alcoholic hepatitis and cirrhosis (AST > ALT), liver abscess, metastatic or primary liver cancer; nonalcoholic steatohepatitis; right heart failure, ischemia or hypoxia, injury to liver ("shock liver"), extensive trauma. Drugs that cause cholestasis or hepatotoxicity. • Decreased in: Pyridoxine (vitamin B6) deficiency. • ALT is the preferred enzyme for evaluation of liver injury.
Alkaline phosphatase • serum • 41–133 IU/L • [0.7–2.2 mckat/L] (method- and age-dependent) • Physiologic Basis: • Alkaline phosphatases are found in liver, bone, intestine, and placenta. • Interpretation • Increased in: Obstructive hepatobiliary disease, bone disease (physiologic bone growth, Paget disease, osteomalacia, osteogenic sarcoma, bone metastases), hyperparathyroidism, rickets, benign familial hyperphosphatasemia, pregnancy (third trimester), GI disease (perforated ulcer or bowel infarct), hepatotoxic drugs. • Decreased in: Hypophosphatasia • Alkaline phosphatase performs well in measuring the extent of bone metastases in prostate cancer.
Bilirubin • 0.1–1.2 mg/dL • [2–21 mcmol/L] • Direct (conjugated to glucuronide) bilirubin: 0.1–0.4 mg/dL [<7 mcmol/L]; • Indirect (unconjugated) bilirubin: 0.2–0.7 mg/dL [<12 mcmol/L] • Physiologic Basis • Bilirubin, a product of hemoglobin metabolism, is conjugated in the liver to mono- and diglucuronides and excreted in bile. • Some conjugated bilirubin is bound to serum albumin, so-called D (delta) bilirubin. • Elevated serum bilirubin occurs in liver disease, biliary obstruction, or hemolysis. • Interpretation • Increased in: Acute or chronic hepatitis, cirrhosis, biliary tract obstruction, toxic hepatitis, neonatal jaundice, congenital liver enzyme abnormalities (Dubin-Johnson, Rotor, Gilbert, Crigler-Najjar syndromes), fasting, hemolytic disorders. Hepatotoxic drugs. • Only conjugated bilirubin appears in the urine, and it is indicative of liver disease; hemolysis is associated with increased unconjugated bilirubin.
Pancreatic Enzymes • Are used to determine the health and function of the pancreas and other areas of the GI system • You measure the native enzymes that are produced by and released by the pancreas. • They include: • Amylase • Lipase
Amylase • serum • 20–110 U/L • [0.33–1.83 mckat/L] (laboratory-specific) • Physiologic Basis • Amylase hydrolyzes complex carbohydrates. • Serum amylase is derived primarily from pancreas and salivary glands and is increased with inflammation or obstruction of these glands. • Interpretation • Increased in: Acute pancreatitis (70–95%), pancreatic pseudocyst, pancreatic duct obstruction (cholecystitis, choledocholithiasis, pancreatic carcinoma, stone, stricture, duct sphincter spasm), bowel obstruction and infarction, mumps, parotitis, diabetic ketoacidosis, penetrating peptic ulcer, peritonitis, ruptured ectopic pregnancy, macroamylasemia. Drugs: azathioprine, hydrochlorothiazide. • Decreased in: Pancreatic insufficiency, cystic fibrosis. Usually normal or low in chronic pancreatitis. • Serum lipase is an alternative test for acute pancreatitis.
Lipase • serum • 0–160 U/L • [0–2.66 mckat/L] (laboratory-specific) • Physiologic Basis • Lipases are responsible for hydrolysis of glycerol esters of long-chain fatty acids to produce fatty acids and glycerol. • Lipases are produced in the liver, intestine, tongue, stomach, and many other cells. • Interpretation • Increased in: Acute, recurrent, pancreatic pseudocyst, pancreatic malignancy, peritonitis, biliary disease, hepatic disease, diabetes mellitus (especially diabetic ketoacidosis), intestinal disease, gastric malignancy or perforation, cystic fibrosis, inflammatory bowel disease (Crohn disease and ulcerative colitis). • Serum lipase may be a more reliable test than serum amylase for the initial diagnosis of acute pancreatitis, due to an increased sensitivity in acute alcoholic pancreatitis and because lipase remains elevated longer than amylase.
Lipase • The specificity of lipase and amylase in acute pancreatitis is similar, though both are poor. Simultaneous measurement of serum amylase and lipase does not improve diagnostic accuracy. Measurement of serum lipase does not help in determining the severity or etiology of acute pancreatitis, and daily measurements are of no value in assessing the patient's clinical progress or ultimate prognosis. • Test sensitivity is not very good for chronic pancreatitis or pancreatic cancer.
Calcium • serum (Ca2 +) • 8.5–10.5 mg/dL • [2.1–2.6 mmol/L] • Panic: <6.5 or >13.5 mg/dL • Physiologic Basis • Serum calcium is the sum of ionized calcium plus complexed calcium and calcium bound to proteins (mostly albumin). • Level of ionized calcium is regulated by parathyroid hormone and vitamin D. • Interpretation • Increased in: Hyperparathyroidism, malignancies secreting parathyroid hormone–related protein (PTHrP) (especially squamous cell carcinoma of lung and renal cell carcinoma), vitamin D excess, milk-alkali syndrome, multiple myeloma, Paget disease of bone with immobilization, sarcoidosis, other granulomatous disorders, familial hypocalciuria, vitamin A intoxication, thyrotoxicosis, Addison disease. Drugs: antacids (some), calcium salts, chronic diuretic use (eg, thiazides), lithium, others.
Calcium • Decreased in: Hypoparathyroidism, vitamin D deficiency, renal insufficiency, pseudohypoparathyroidism, magnesium deficiency, hyperphosphatemia, massive transfusion, hypoalbuminemia. • Need to know serum albumin to interpret calcium level. For every decrease in albumin by 1 mg/dL, calcium should be corrected upward by 0.8 mg/dL.