Download
1 / 1
10 likes | 145 Vues
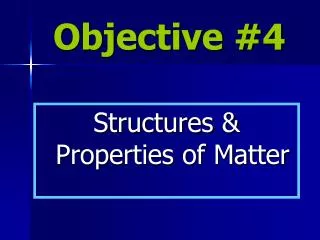
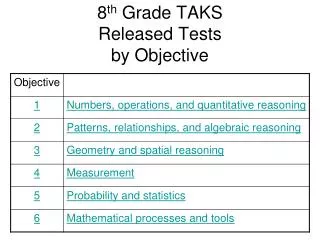
Figure 1. 1.0. 0.9. 0.8. 0.7. Disease Free Survival. 0.6. S S+RT. p = 0.59. 0.5. Fraction Surviving. 0.4. Overall Survival. S S+RT. p = 0.92. 0.3. 0.2. 0.1. 0.0. 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. Time, years.

E N D
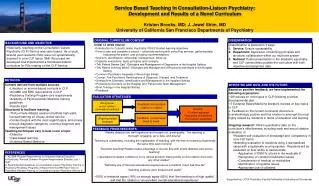
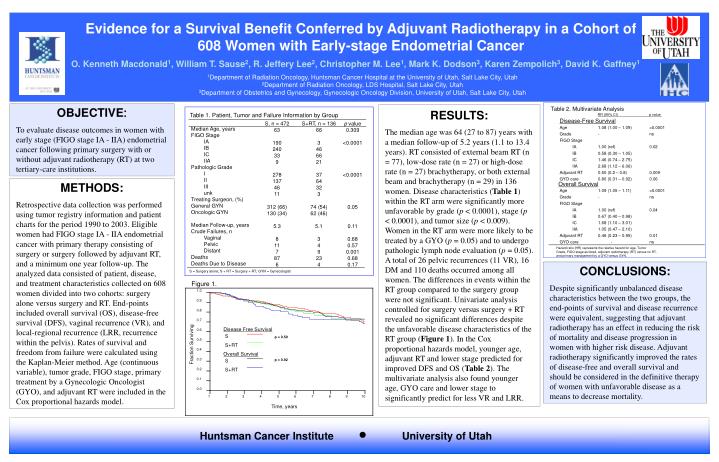
Figure 1. 1.0 0.9 0.8 0.7 Disease Free Survival 0.6 S S+RT p = 0.59 0.5 Fraction Surviving 0.4 Overall Survival S S+RT p = 0.92 0.3 0.2 0.1 0.0 1 2 3 4 5 6 7 8 9 10 Time, years Evidence for a Survival Benefit Conferred by Adjuvant Radiotherapy in a Cohort of 608 Women with Early-stage Endometrial Cancer O. Kenneth Macdonald1, William T. Sause2, R. Jeffery Lee2, Christopher M. Lee1, Mark K. Dodson3, Karen Zempolich3, David K. Gaffney1 1Department of Radiation Oncology, Huntsman Cancer Hospital at the University of Utah, Salt Lake City, Utah 2Department of Radiation Oncology, LDS Hospital, Salt Lake City, Utah 3Department of Obstetrics and Gynecology, Gynecologic Oncology Division, University of Utah, Salt Lake City, Utah OBJECTIVE: To evaluate disease outcomes in women with early stage (FIGO stage IA - IIA) endometrial cancer following primary surgery with or without adjuvant radiotherapy (RT) at two tertiary-care institutions. RESULTS: The median age was 64 (27 to 87) years with a median follow-up of 5.2 years (1.1 to 13.4 years). RT consisted of external beam RT (n = 77), low-dose rate (n = 27) or high-dose rate (n = 27) brachytherapy, or both external beam and brachytherapy (n = 29) in 136 women. Disease characteristics (Table 1) within the RT arm were significantly more unfavorable by grade (p < 0.0001), stage (p < 0.0001), and tumor size (p < 0.009). Women in the RT arm were more likely to be treated by a GYO (p = 0.05) and to undergo pathologic lymph node evaluation (p = 0.05). A total of 26 pelvic recurrences (11 VR), 16 DM and 110 deaths occurred among all women. The differences in events within the RT group compared to the surgery group were not significant. Univariate analysis controlled for surgery versus surgery + RT revealed no significant differences despite the unfavorable disease characteristics of the RT group (Figure 1). In the Cox proportional hazards model, younger age, adjuvant RT and lower stage predicted for improved DFS and OS (Table 2). The multivariate analysis also found younger age, GYO care and lower stage to significantly predict for less VR and LRR. Table 2. Multivariate Analysis Table 1. Patient, Tumor and Failure Information by Group RR (95% CI) p value Disease-Free Survival S, n = 472 63 190 240 33 9 278 137 46 11 312 (66) 130 (34) 5.3 8 11 7 87 6 S+RT, n = 136 66 3 46 66 21 37 64 32 3 74 (54) 62 (46) 5.1 3 4 9 23 4 p value 0.309 <0.0001 <0.0001 0.05 0.11 0.68 0.57 0.001 0.68 0.17 Age 1.08 (1.00 – 1.09) <0.0001 Grade - ns FIGO Stage IA 1.00 (ref) 0.02 IB 0.58 (0.30 – 1.05) IC 1.46 (0.74 – 2.75) IIA 2.68 (1.12 – 6.06) Adjuvant RT 0.50 (0.2 – 0.8) 0.009 GYO care 0.80 (0.31 – 0.92) 0.06 Median Age, years FIGO Stage IA IB IC IIA Pathologic Grade I II III unk Treating Surgeon, (%) General GYN Oncologic GYN Median Follow-up, years Crude Failures, n Vaginal Pelvic Distant Deaths Deaths Due to Disease METHODS: Retrospective data collection was performed using tumor registry information and patient charts for the period 1990 to 2003. Eligible women had FIGO stage IA - IIA endometrial cancer with primary therapy consisting of surgery or surgery followed by adjuvant RT, and a minimum one year follow-up. The analyzed data consisted of patient, disease, and treatment characteristics collected on 608 women divided into two cohorts: surgery alone versus surgery and RT. End-points included overall survival (OS), disease-free survival (DFS), vaginal recurrence (VR), and local-regional recurrence (LRR, recurrence within the pelvis). Rates of survival and freedom from failure were calculated using the Kaplan-Meier method. Age (continuous variable), tumor grade, FIGO stage, primary treatment by a Gynecologic Oncologist (GYO), and adjuvant RT were included in the Cox proportional hazards model. Overall Survival Age 1.09 (1.05 – 1.11) <0.0001 Grade - ns FIGO Stage IA 1.00 (ref) 0.04 IB 0.67 (0.40 – 0.98) IC 1.68 (1.10 – 3.01) IIA 1.05 (0.47 – 2.10) Adjuvant RT 0.46 (0.23 – 0.95) 0.01 GYO care - ns Hazard ratio (HR) represents the relative hazard for age, Tumor Grade, FIGO stage as listed, adjuvant radiotherapy (RT) versus no RT, and primary management by a GYO versus GYN. CONCLUSIONS: Despite significantly unbalanced disease characteristics between the two groups, the end-points of survival and disease recurrence were equivalent, suggesting that adjuvant radiotherapy has an effect in reducing the risk of mortality and disease progression in women with higher risk disease. Adjuvant radiotherapy significantly improved the rates of disease-free and overall survival and should be considered in the definitive therapy of women with unfavorable disease as a means to decrease mortality. S = Surgery alone; S + RT = Surgery + RT; GYN = Gynecologist ● Huntsman Cancer Institute University of Utah