Download
1 / 54
1.18k likes | 4.6k Vues
Thrombocytopenic purpura. Huang Honghui Dept. of Hematology, Renji Hospital. Definition: Thrombocytopenia is a clinical syndrome in which a decreased number of platelets in the circulating blood present as a bleeding tendency, i.e. skin, mucosa or internal organ bleeding.

E N D
Thrombocytopenic purpura Huang Honghui Dept. of Hematology, Renji Hospital
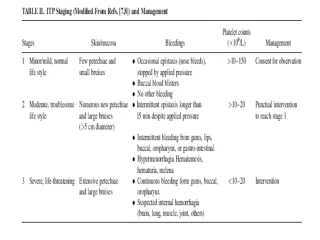
Definition: Thrombocytopenia is a clinical syndrome in which a decreased number of platelets in the circulating blood present as a bleeding tendency, i.e. skin, mucosa or internal organ bleeding. • It is the most common course of abnormal bleeding(30%). • Classification: idiopathic/ secondary
BPC<50000/μl----bleeding tendency • BPC<20000/μl----spontaneous hemorrhage
Definition • ITP is an acquired disease of children and adults characterized by a low platelet count, an normal or increased numbers of megakaryocytes in the bone marrow, and absence of evidence for other disease.
Classification • Acute type (aITP) • Chronic type (cITP)
Etiology and Pathogenesis • Infection(bacteria or virus) • aITP--- antecedent viral infection • cITP--- state of illness worsen because of infection • anti-viral antibody or immunocomplex in plasma
Etiology and Pathogenesis • Immunologic processes • The infusion of plasma from patients with ITP into normal recipients → thrombocytopenia • The infusion of normal platelets into patients with ITP → destructed within 12-24h • platelet associated antibodies ( PAIgG, PAIgA, PAIgM ) • Glucocorticoid, plasmapheresis, HD-Ig --- good response
Etiology and Pathogenesis • Role of the liver and spleen • The site of production of platelet antibodies. • The site of platelet clearance. • Splenic sequestration is the major site of platelet clearance in ITP.( 51Cr-labeled isologous platelet ) • Hepatic sequestration ---- severe thrombocytopenia and markedly shorten platelet survival.
Etiology and Pathogenesis 51Cr labeled isologous platelet Administrate to patients with ITP External scintillation counting Rapid accumulation of radioactivity predominantly in the spleen Splenic sequestration is the major site of platelet clearance in ITP
Etiology and Pathogenesis • Others • Impaired thrombopoiesis • In cITP, an Ig has been demonstrated on the surface of the megakaryocytes →the attachment of antibody may impair platelet production.
Etiology and Pathogenesis • Others • Role of estrogenic hormones • Suppress the platelet production. • Stimulate the clearance ability of monocyte-macrophage against the antibody binding platelet.
Clinical Features • Acute ITP • Most frequently in children 2 to 6 years. • A history of viral infection preceding the onset of bleeding. • Acute onset.
Clinical Features • The symptoms and signs of bleeding: • Bruises and petechiae are the nearly universal presenting clinical symptom. • <1/3: epistaxis and gingival bleeding. • <10%: hematuria, gastrointestinal bleeding. • <3%: severe (massive purpura, profuse epistaxis and retinal hemorrhages.) • Self-limited, spontaneous remission.
Clinical Features • Chronic ITP • More frequently in females(<40yrs), F:M=4:1. • Insidious onset.
Clinical Features • The symptoms and signs of bleeding: • Petechiae: asymptomatic, not palpable, most in dependent regions. • Purpura • Menorrhagia • Epistaxis,gingival bleeding • Gastrointestinal bleeding and hematuria are less common. • Intracerebral hemorrhage is uncommon,but it is the most common cause of death. • Fluctuating course,spontaneous remission is uncommon.
Clinical Features • Others • Anemia: iron deficiency type. • Splenomegaly
Laboratory Finding • Blood • Platelet count • Acute type <20×109/L • Chronic type 30-80×109/L • Morphology and function of platelet • Morphology:abnormal large, “giant” forms, bizarre shapes, deeply stained forms. • Functions:adhesion N/↓, aggregation N/↓ • Others: • Hb: N/↓ • WBC: normal/eosinophilia
Laboratory Finding • Bone marrow • megakaryocytes increased or normal. • disturbance of development and maturation: immature megakaryocytes↑, granule in cytoplasm ↓,size ↓. • platelet-producing megakaryocyte↓(<30%)
Megakaryoblast0%Promegakaryocyte0-5%Granular megakaryocyte10-27%Platelet-producing megakaryocyte44-60%Platelet
1.Megakaryoblast 2.Promegakaryocyte 3.Granular Megakaryocyte Acute ITP(BM)
1.Granular megakaryocyte 6.Megakaryoblast in metaphase of mitosis 7.Giant platelets Chronic ITP(BM)
Laboratory Finding • Platelet associated antibodies and complements • Assay of PAIgG and PAC3 • PAIgG: • the first sensitive and reproducible method • increased • The magnitude of increase is greater in patients with more severe thrombocytopenia.
Laboratory Finding • Others • Platelet survival time (51Cr labeled) • Normal: 7-11days • Acute type: 1-6 hour • Chronic type: 1-3 day
Laboratory Finding • Others • Tests of hemostasis and blood coagulation • Bleeding time: prolonged; • Clot retraction: absent or deficient; • PT, PTT, CT: normal
Diagnosis and Differential Diagnosis • Diagnostic criteria • bleeding manifestation • BPC count ↓ • No or mild splenomagaly • megakaryocytes increased or normal, having disturbance of maturation • Anyone of the followings • Response to glucocorticoid • Response to splenetomy • PAIg(+) • PAC3(+) • Platelet survival time ↓
Diagnosis and Differential Diagnosis • Exclude secondary thrombocytopenia • Such as: acute infectious illness, myelodysplastic syndrome, hypersplenism, disseminated intravascular coagulation, aplastic anemia, acute leukemia, systemic lupus erythematous.
Treatment • Supporting measure • Observation • Glucocorticoids • Splenectomy • Immunosuppressive drugs • Others • Emergency treatment
Treatment:(1)Supporting measure • Supporting measure • Physical activity should be restricted to minimize the hazards of trauma, particularly head injury. • Drugs that impair platelet functions should be avoided. • Blood loss should be treated as otherwise indicated.
Treatment:(2)Observation • Observation • Platelet count > 50×109/L and • Asymptomatic or have only minor purpura
Treatment:(3)Glucocorticoids • Mechanism of action: • significantly diminish immunoglobulin synthesis. • inhibit the binding of antibodies to platelets. • impair reticuloendothelial function and thereby to diminish platelet destruction. • Improve the permeability of capillary • Stimulate the hematopoisis and accelerate the release of platelet into peripheral blood.
Treatment:(3)Glucocorticoids • Initial means of therapy • Response rate: 60-90% • Dosage and regimen • Prednisone 1-2mg/kg.d p.o. • The initial course of glucocorticoids should be maintained for 3 to 4 weeks, followed by a gradual tapering of the dosage. • Therapy course: 6 months
Treatment:(4)Splenectomy • Mechanism of action • Removal of the major site of destruction of antibody-sensitized platelets. • Removal of a major site of antibody synthesis.
Treatment:(4)Splenectomy • Indications • failure to respond to glucocorticoid therapy, relapse after discontinuance of glucocorticoid therapy or reduction in the dosage. • the necessity of high doses of glucocorticoid for maintenance of a clinical status free of serious hemorrhage. • overriding contraindications due to the use of glucocorticoids. • Radioactivity index of spleen ↑(51Cr)
Treatment:(4)Splenectomy • Contraindications • in children under 2 years of age • in many cases of ITP in pregnant women. • in patients with cardiac or other complications who are at risk of serious sequelae from any major surgical procedure.
Treatment:(5)Immunosuppressive drugs • Indications • Failure to response to glucocorticoid therapy and splenectomy • Contraindications due to glucocorticoid therapy and splenectomy • Combined therapy with glucocorticoid in order to improve and decrease the dose of glucocorticoid
Treatment:(5)Immunosuppressive drugs • Vincristine: 0.025mg/kg i.v. Qw×4-6w (total dose <2mg) • Cyclophosphamide: 50-100mg/day orally ×3-6w or 400-600 mg i.v. Q3-4w • Azathioprine: 100-200mg/d p.o. ×3-6w → 25-50mg/d p.o. ×8-12w • CSA: 250-500mg/d p.o. ×3-6w → 50-100mg/d p.o. ×6m
Treatment:(6)Others • Danazol: androgen with minimal virilizing side effects • Mechanism of action • induce reticuloendothelial dysfunction, possibly by diminishing Fc (IgG) receptors. • Anti-estrogen effect. • Dosage:0.3-0.6g/d×2-3m • Side effect: liver function abnormality, headache, nausea, etal.
Treatment:(6)Others • Rh Immune Globulin • Mechanism of Action • phagocytic cell blockade due to occupancy of the phagocytic cell Fc receptors by the IgG-sensitized RBCs • Dosage • The probability of response increases with the dose administered. • A common regimen administers 25 µg/kg of anti-D intravenously and repeats the same dose 2 days later if no or minimal response is evident.
Treatment: (7)Emergency treatment • Indications: • platelet count <20×109/L, • severe life-threatening bleeding • serious complications, e.g., intracranial hemorrhage • immediate preoperative treatment of patients or pregnant women with serious hemorrhage
Treatment:(7)Emergency treatment • Platelet transfusions • produce some increase in platelet numbers • diminish bleeding for a time • should be avoided in patients with chronic ITP
Treatment: (7)Emergency treatment • High-dose immunoglobulin • Mechanism of action • blockade of the Fc receptors of the reticuloendothelial cells • neutralization of antiplatelet autoantibodies by antiidiotypic antibodies in the preparations • Regimen: 400mg/kg/day for 5 days • Response rate: 60-80%