Download
1 / 1
10 likes | 226 Vues
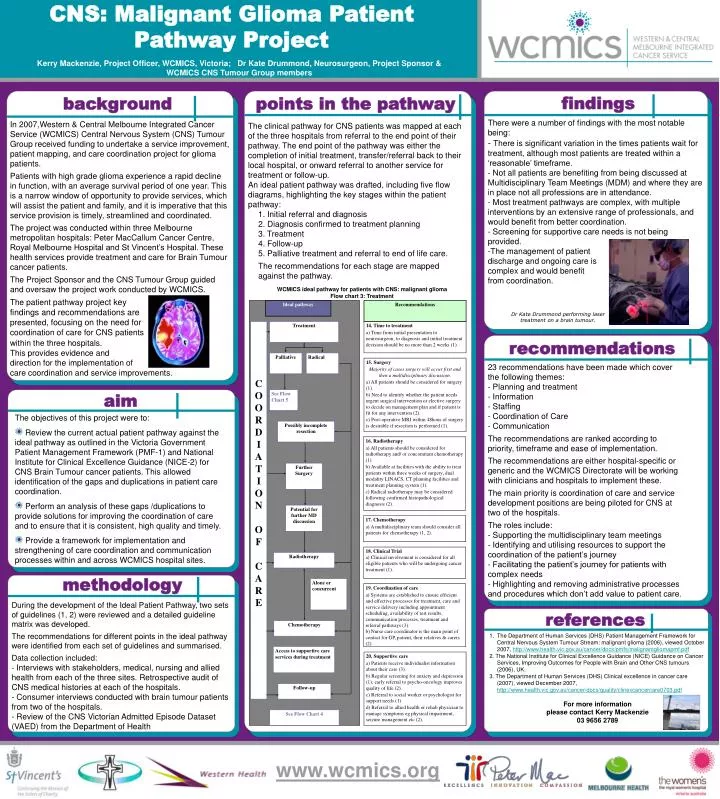
CNS: Malignant Glioma Patient Pathway Project. Ideal pathway. Recommendations. C O O R D I A T I O N O F C A R E. Treatment. 14. Time to treatment

E N D
CNS: Malignant Glioma Patient Pathway Project Ideal pathway Recommendations C O O R D I A T I O N O F C A R E Treatment 14. Time to treatment a) Time from initial presentation to neurosurgeon, to diagnosis and initial treatment decision should be no more than 2 weeks (1). Palliative Radical 15. Surgery Majority of cases surgery will occur first and then a multidisciplinary discussion. a) All patients should be considered for surgery (1). b) Need to identify whether the patient needs urgent surgical intervention or elective surgery to decide on management plan and if patient is fit for any intervention (2). c) Post-operative MRI within 48hous of surgery is desirable if resection is performed (1). See Flow Chart 5 Possibly incomplete resection 16. Radiotherapy a) All patients should be considered for radiotherapy and/ or concomitant chemotherapy (1). b) Available at facilities with the ability to treat patients within three weeks of surgery, dual modality LINACS, CT planning facilities and treatment planning system (1). c) Radical radiotherapy may be considered following confirmed histopathological diagnosis (2). Further Surgery Potential for further MD discussion 17. Chemotherapy a) A multidisciplinary team should consider all patients for chemotherapy (1, 2). 18. Clinical Trial a) Clinical involvement is considered for all eligible patients who will be undergoing cancer treatment (1). Radiotherapy Alone or concurrent 19. Coordination of care a) Systems are established to ensure efficient and effective processes for treatment, care and service delivery including appointment scheduling, availability of test results, communication processes, treatment and referral pathways (3). b) Nurse care coordinator is the main point of contact for GP, patient, their relatives & carers (2). Chemotherapy Access to supportive care services during treatment 20. Supportive care a) Patients receive individualist information about their care (3). b) Regular screening for anxiety and depression (1); early referral to psycho-oncology improves quality of life (2). c) Referral to social worker or psychologist for support needs (1) d) Referral to allied health or rehab physician to manage symptoms eg physical impairment, seizure management etc (2). Follow-up See Flow Chart 4 Kerry Mackenzie, Project Officer, WCMICS, Victoria; Dr Kate Drummond, Neurosurgeon, Project Sponsor & WCMICS CNS Tumour Group members findings background points in the pathway • There were a number of findings with the most notable being: • - There is significant variation in the times patients wait for treatment, although most patients are treated within a ‘reasonable’ timeframe. • - Not all patients are benefiting from being discussed at Multidisciplinary Team Meetings (MDM) and where they are in place not all professions are in attendance. • - Most treatment pathways are complex, with multiple interventions by an extensive range of professionals, and would benefit from better coordination. • - Screening for supportive care needs is not being provided. • The management of patient • discharge and ongoing care is • complex and would benefit • from coordination. In 2007,Western & Central Melbourne Integrated Cancer Service (WCMICS) Central Nervous System (CNS) Tumour Group received funding to undertake a service improvement, patient mapping, and care coordination project for glioma patients. Patients with high grade glioma experience a rapid decline in function, with an average survival period of one year. This is a narrow window of opportunity to provide services, which will assist the patient and family, and it is imperative that this service provision is timely, streamlined and coordinated. The project was conducted within three Melbourne metropolitan hospitals: Peter MacCallum Cancer Centre, Royal Melbourne Hospital and St Vincent’s Hospital. These health services provide treatment and care for Brain Tumour cancer patients. The Project Sponsor and the CNS Tumour Group guided and oversaw the project work conducted by WCMICS. The patient pathway project key findings and recommendations are presented, focusing on the need for coordination of care for CNS patients within the three hospitals. This provides evidence and direction for the implementation of care coordination and service improvements. • The clinical pathway for CNS patients was mapped at each of the three hospitals from referral to the end point of their pathway. The end point of the pathway was either the completion of initial treatment, transfer/referral back to their local hospital, or onward referral to another service for treatment or follow-up. • An ideal patient pathway was drafted, including five flow diagrams, highlighting the key stages within the patient pathway: • 1. Initial referral and diagnosis • 2. Diagnosis confirmed to treatment planning • 3. Treatment • 4. Follow-up • 5. Palliative treatment and referral to end of life care. • The recommendations for each stage are mapped against the pathway. • WCMICS ideal pathway for patients with CNS: malignant glioma • Flow chart 3: Treatment Dr Kate Drummond performing laser treatment on a brain tumour. recommendations 23 recommendations have been made which cover the following themes: - Planning and treatment - Information - Staffing - Coordination of Care - Communication The recommendations are ranked according to priority, timeframe and ease of implementation. The recommendations are either hospital-specific or generic and the WCMICS Directorate will be working with clinicians and hospitals to implement these. The main priority is coordination of care and service development positions are being piloted for CNS at two of the hospitals. The roles include: - Supporting the multidisciplinary team meetings - Identifying and utilising resources to support the coordination of the patient’s journey - Facilitating the patient’s journey for patients with complex needs - Highlighting and removing administrative processes and procedures which don’t add value to patient care. aim • The objectives of this project were to: • Review the current actual patient pathway against the ideal pathway as outlined in the Victoria Government Patient Management Framework (PMF-1) and National Institute for Clinical Excellence Guidance (NICE-2) for CNS Brain Tumour cancer patients. This allowed identification of the gaps and duplications in patient care coordination. • Perform an analysis of these gaps /duplications to provide solutions for improving the coordination of care and to ensure that it is consistent, high quality and timely. • Provide a framework for implementation and strengthening of care coordination and communication processes within and across WCMICS hospital sites. methodology During the development of the Ideal Patient Pathway, two sets of guidelines (1, 2) were reviewed and a detailed guideline matrix was developed. The recommendations for different points in the ideal pathway were identified from each set of guidelines and summarised. Data collection included: - Interviews with stakeholders, medical, nursing and allied health from each of the three sites. Retrospective audit of CNS medical histories at each of the hospitals. - Consumer interviews conducted with brain tumour patients from two of the hospitals. - Review of the CNS Victorian Admitted Episode Dataset (VAED) from the Department of Health references • The Department of Human Services (DHS) Patient Management Framework for Central Nervous System Tumour Stream: malignant glioma (2006), viewed October 2007, http://www.health.vic.gov.au/cancer/docs/pmfs/malignantgliomapmf.pdf • 2. The National Institute for Clinical Excellence Guidance (NICE) Guidance on Cancer Services, Improving Outcomes for People with Brain and Other CNS tumours (2006), UK. • 3. The Department of Human Services (DHS) Clinical excellence in cancer care (2007), viewed December 2007, http://www.health.vic.gov.au/cancer/docs/quality/clinexcancercare0703.pdf • For more information • please contact Kerry Mackenzie • 03 9656 2789