Download
1 / 22
291 likes | 899 Vues
Feeding Tube Placements: Dietitian training and the Procedure. Lisa Molnar, RD, LD, CNSC Hennepin County Medical Center (HCMC). Objectives. After this presentation the attendee should be able to Develop training for dietitians to place feeding tubes at their facility

E N D
Feeding Tube Placements:Dietitian training and the Procedure Lisa Molnar, RD, LD, CNSC Hennepin County Medical Center (HCMC)
Objectives • After this presentation the attendee should be able to • Develop training for dietitians to place feeding tubes at their facility • Understand the procedure of feeding tube placement at the bedside.
Dietitian Feeding Tube placements at HCMC • Started in June of 2011 • Primary placer in the MICU, SICU, BURN, and PICU, Monday – Friday 8am-4pm • Each floor has own rules for nursing placement • Back up placer in all other areas of the hospital during same hours • Float Pool RN is primary contact 24/7 on floors • After hours/weekend/holiday if available, but not staffed • 5 Dietitians • 2 Full Time • 3 Part Time (0.6, 0.5, and 0.7) • Use the Cortrak® Monitor • Avg. 50-60 patients/placements per month • Currently, no change in staffing or work loads
Feeding Tube Data April-December 2012, N=489 • Average length of time from order placement to response: 5 ½ hours • Delayed 2/2 other procedures, weekend/night orders, hemodynamic instability of patient • Average Length of time of feeding tube placement: 23 minutes • Actual placement time (not including set up/clean up) • 85% Small Bowel placement • 78% Nasal Bridle use • Average number of X-rays per feeding tube placement: 1.15 • Reglan use: 38% of placements
Feeding Tube Placement Competency At HCMC • Review Hospital Policies • Feeding Tube Placement and Enteral Feeding • Review Readings • Mosby’s Nursing Skills • Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient: Society of Critical Care Medicine (SCCM) • American Dietetic Association’s Evidenced Analysis Library, Critical Illness topics: gastric vs small bowel feeding tube placement; Monitoring criteria in critical care: gastric residual volume, patient positioning, promotility agents • Nutrition Critical Care Clinical Practice Guidelines. Strategies to Optimize Delivery and Minimize Risk of EN. • View videos on feeding tube placement • Corpak® Video • Cortrak® Video • Observe feeding tube placement in Fluoroscopy x 1-2 • Review directions for use of the Cortrak® device and observe RD/RN place gastric and small bowel feeding tubes using Cortrak® until comfortable with the procedure • On the job training with trained RD/ICU RN with successful placement of at least 3 in small bowel
Training with Corpak® Medsystems • Cortrak® sent out a nurse to assist with Training for 1 week after complete non-hands on portion of competency • Completed slide show education with the nurse from Cortrak® • Hands on training – placed as many feeding tubes as ordered during that week in SICU and MICU with observation of Cortrak® nurse • Minimum for 3 successfully before deemed “competent” • After “competent”, must complete 1 feeding tube placement successfully every 3 months to maintain competency
Training new Dietitians • Same competency form • New dietitian will shadow competent dietitian placing feeding tubes until comfortable to start placing on own • New dietitian will place at least 3 post pyloric feeding tubes successfully with observation until dietitian is comfortable.
Check List before starting • Check physician order • Nasal vs Oral Placement • Gastric vs post-pyloric • Communicate with primary RN • Timing • Sedation needed • Pro-kinetic agent (ieReglan) • Explain procedure to the patient/family
Feeding Tube Placement – Set up • Obtain Supplies • Feeding tube • 10 Fr in adults (43 in or 55 in) • 8 Fr in peds (36 in) • Cortrak® Monitor • 10 mL saline flush • 60 mLluer or eccentric tip syringe • Lubrication • Stethoscope • Nasal Bridle or Tape • AMT Bridle® • NGT tape • Paper Tape, Silk Tape (to patient or ETT) • Twill Tape
Cortrak® Monitor Feeding tube wire connects to monitor Monitor Place over Zyphoid Process
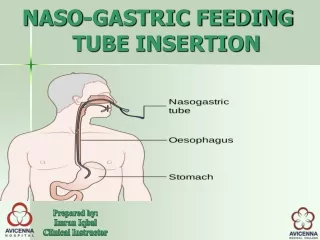
Getting Started • Place Cortrak® monitor device over Zyphoid Process, the device should be level • Enter via nare or mouth depending on order • Once feeding tube advanced to 5-10 cm, turn Cortrak® monitor on • Watch monitor as advance feeding tube • Feeding tube should go straight down to cross section • If deviates left or right prior to cross section, possible lung placement
Getting to the Stomach • Most adults GE junction is at 50 cm, can measure if peds or abnormal sized adult • Auditory confirmation by pushing air through 60 mL syringe and listening with a stethoscope • Advance feeding tube to desired final location • Ok to push (give length) through the stomach. • If having trouble • Pull NGT • Fill stomach with air • Pull out stylet a few inches and try to advance • Turn the tube as advancing • Go slower
Getting post pyloric • The longest portion of the feeding tube placement • Do not advance in length, put pressure on the tube only, small intestine will pull it in • Tips to improve advancement • “Floppy tip” – pulling out the stylet • Flush with saline or air • Reglan use (IV 10 mg works in minutes) • Turn the tube while putting on pressure • Reposition the patient • Pull back/out NGT
Secure the feeding tube NGT Tape Nasal Bridle Twill Tape