Download
1 / 8
80 likes | 105 Vues
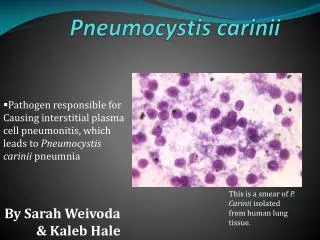
Pneumocystis prophylaxis in ANCA v asculitis Robert Hunter Wellcome Trust Clinical Research Career Development Fellow Honorary Consultant In Renal Medicine @renalrob. Pneumocystis prophylaxis in ANCA vasculitis. Overview : Risk of PCP in ANCA vasculitis A case P rophylaxis regimens

E N D
Pneumocystis prophylaxis in ANCA vasculitis Robert Hunter Wellcome Trust Clinical Research Career Development Fellow Honorary Consultant In Renal Medicine @renalrob
Pneumocystis prophylaxis in ANCA vasculitis • Overview: • Risk of PCP in ANCA vasculitis • A case • Prophylaxis regimens • Trimethoprim-sulfamethoxazole desensitisation • Questions: • Who should receive PCP prophylaxis? • What should we do when patients are allergic to TMP-SMX?
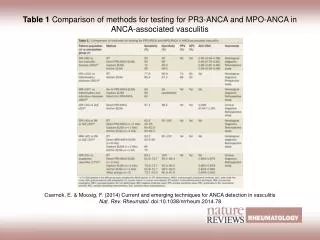
Jarrousse (1993) PCP in ANCA vasculitis Guillevin (1997) Reinhold-Keller (2000) Bligny (2002) Booth (2003) Charles (2011) Guillevin (2014) Edinburgh registry
Case Case of PCP in patient with AAV during maintenance rituximab. Role of T-S desensitisation discussed.
PCP prophylaxis Options: 1) trimethoprim-sulfamethoxazole (daily, thrice-weekly) 2) dapsone 100 mg daily 3) dapsone 100 mg + pyrimethamine 25 mg twice-weekly 4) atovaquone 750 mg daily 5) pentamidine 300 mg nebulised monthly NB dose-adjustments in renal failure and potential interaction between methotrexate and TMP-SMX
TMP-SMX prophylaxis • TMP-SMX is effective at preventing PCP • (Stern et al., Cochrane Rev, 2016) • Adverse reactions lead to discontinuation of TMP-SMX in ~20% • Desensitisation is more effective than re-challenge • (Lin et al., Cochrane Rev, 2007) • Our desensitisation regime: • 96 mg daily for 3 days (= 1 ml of 480 mg / 5 ml liquid) • 192 mg for 3 days (= 2 ml) • 288 mg for 3 days (= 3 ml) • 384 mg for 3 days (= 4 ml) • 480 mg daily (= 5 ml or convert to tablet)
Our answers • Who should receive PCP prophylaxis? • everybody during induction (not only cyclophosphamide) • …and for months-years thereafter • inclusive (vs. risk-oriented) prescription • possible immunomodulatory benefit of TMP-SMX • (Stegemanet al., NEJM 1996; Salmela et al., Rheumatology, 2017) • What should we do when patients are allergic to TMP-SMX? • consider immune context • desensitise (13-day regime, steroids, anti-histamines, close monitoring)
Acknowledgments • Neeraj Dhaun (Bean) • BHFIntermediate Fellow & Honorary Consultant Nephrologist • David Kluth • Senior Lecturer in Nephrology & Honorary Consultant Nephrologist • Eve Miller-Hodges • Specialist Registrar in Nephrology & Vasculitis Fellow • Tariq Farrah • MRCClinical Fellow • Jin Werne Hah • Renal Pharmacist • Sadaf Arshad • Renal Pharmacist @renalrob