Download
1 / 15
190 likes | 478 Vues
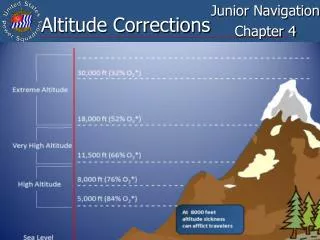
Exercise and Altitude. Moderate altitude 1500m (5000ft) Dec max O2 consumption Extreme altitude 6000m(20000ft) Progressive deterioration - death Fig 23-1 less O2 available As barometric pressure decreases Less O2 per volume - same % as sea level Table 23-1 Acute exposure

E N D
Exercise and Altitude • Moderate altitude 1500m (5000ft) • Dec max O2 consumption • Extreme altitude 6000m(20000ft) • Progressive deterioration - death • Fig 23-1 less O2 available • As barometric pressure decreases • Less O2 per volume - same % as sea level • Table 23-1 Acute exposure • Still see dec in O2 tx capacity at higher and higher altitudes • Fig 23-3 effect of altitude on VO2 max • 3% decline / 300m (1000ft) • O2 cost is similar - perception of effort is greater - higher % of max
Human Responses • With proper acclimatization humans can tolerate high altitudes • Table 23-2 - ability to adapt • Slow ascent to 5500m (18000ft) can be accomplished with few symptoms • If ascent is rapid -AMS -acute mountain sickness - within a few hours • Headache, nausea, irritability, weakness, poor appetite, vomiting, tachycardia, disturbed breathing • Above 3000m AMS common • Blunted breathing response more susceptible • Slow ascent can reduce AMS • Acclimation hikes important
Pulmonary Function • Ventilation inc further for 2 weeks • Hypoxia is driving force (fig 23-4) • Bicarb is excreted - inc central and peripheral sensitivity • HVR - hypoxic ventilatory response • Important to maintain Alv and Art O2 • Determines Max O2 consumption • Elite athletes - often blunted HVR • Observe dec in PaO2 with intense ex • May be pulmonary gas exchange • Diffusion limitation at altitude • Partial P of O2 determines driving force • O2 cascade(fig 23-5) • Fig 23-6 - same transit time - dec driving force (slope)
Cardiovascular Adjustments • Acute - submax HR inc - SV ~ same • Chronic • SV dec, CO dec 20-25% (1-2 weeks) • Fig 23-7 • MAP - mean arterial BP - gradually inc with exposure • Due to inc systemic resistance and vascular resistance in ms • Due to inc bld viscosity and catecholamines • Above 3000m EPO stimulates Hb and Hct - requires ~ 3 months • Time reduced with adequate energy, protein and iron
Acclimatization • Rate Pressure Product - work load on heart (HR * Systolic BP) • Inc 100% above 3000m (exercise) • Significant challenge to heart • Lungs - PAP - pulmonary Arterial P • Inc with altitude - symp stimulation • Inc size of sm ms in pulmonary arterioles • Implicated in HAPE (pulmonary edema) • Brain - hypoxemia - vasodilation • Implicated in HACE (cerebral edema) • Hypocapnea - vasoconstriction • Counteracats vasodilation
Muscle Acclimatization • Dec submax bld flow (20-25%) • Due to inc Nep and dec CO • O2 delivery maintained - through inc O2 content in blood • Inc myoglobin, buffering capacity, aerobic enzymes (small change) • Oxidative capacity • Altitude native - low mito volume • Activity limited by pulmonary vent • Even unfit have sufficient Ox capacity at altitude • Endurance capacity inc with acclimatization (no change in VO2 max)
Nutrition and Energetics • Weight loss and ms atrophy common • 100-200 g/day - dehydration, energy deficit, inc activity level, inc BMR • High carb diet can help > 60% • Exercise Energetics • Lactate paradox - fig 23-8 • Bld lactate higher at given power output with acute exposure • Acclim - dec bld lactate but no change in max O2 consumption • Fig 23-9 • With acclimatization • Dec Ep, Nor Ep stays high • Working ms oxidizes more of its own lactate - inc dependence on bld glucose
Metabolism • Carbohydrates - thought to be preferred fuel - higher yield of ATP/O2 • Limited storage • Hypoglycemia and liver glycogen depletion • Reduced with high carbohydrate diet • Fat and Protein • Inc fat catabolism if diet is inadequate - glucose preferred
Athletics at Altitude • Table 23--3 • Improvements in short duration, high intensity activities • Reduced gravity and wind resistance • Decreased endurance performance - longer than 800m • Athletes benefit from 1-12 weeks of acclimatization • Problem - reduced absolute training intensity at altitude - even if same % • Can not train as hard - detraining effect • Further - do not see improvements in sea level performance (reduction) • Reduced bld volume, buffering capacity, inc ventilation (more work)
Live High - Train Low • Combine benefits of sedentary adaptations to altitude • With maximal training stimulus at sea level • Either live 2200-3500m and drive down every day to train • Or sleep in hypoxic tent - reduced oxygen tension • Stimulates adaptation