Download
1 / 99
1.04k likes | 1.64k Vues
Introduction to ACAM2000 Smallpox Vaccine. David Wonnacott, PhD Senior Vice President of Quality and Regulatory. Acambis Overview. Acambis develops novel vaccines to prevent and treat infectious diseases Acambis locations: Cambridge, UK (Head Office) – Canton, MA (manufacturing)

E N D
Introduction to ACAM2000 Smallpox Vaccine David Wonnacott, PhD Senior Vice President of Quality and Regulatory
Acambis Overview • Acambis develops novel vaccines to prevent and treat infectious diseases • Acambis locations: • Cambridge, UK (Head Office) – Canton, MA (manufacturing) • Cambridge, MA (R&D) – Rockville, MD (lyophilization, fill/finish) • 200+ employees
“Answering The Call” • Critical demand for new and improved smallpox vaccine • Commercial manufacturing ceased after elimination of disease (1970’s) • Strategic National Stockpile required new source of vaccine • ACAM2000 is unique • Needed to establish safety and efficacy in absence of disease • Highly targeted use managed by government agencies
Manufacturing Original Bioreactor Calf skin vaccines, begun in 1805 Today’s Bioreactor ACAM2000, 2001 - ongoing
Parallel Clinical Development and Manufacturing Timeline for Smallpox Vaccine (ACAM2000) 192.5 million doses delivered to SNS* Terrorist and anthrax attacks CDC contract awarded to Acambis Fast Track Designation 9/11 and 10/01 11/01 12/02 12/04 12/06 8/02 10/02 2/05 8/06 IND filed Clinical trial program (Phase I - III) BLA filed * SNS – Strategic National Stockpile
History of Smallpox Disease, Vaccination, and Eradication John Neff, MD Seattle Children’s Hospital and Regional Medical Center
Topics to be Covered • History of Smallpox • Control, eradication, and potential for bioterrorism use • Smallpox Vaccination • Development, protection, adverse events • Description of Smallpox • Clinical types and expected mortality • Conclusions
Overview of Smallpox • First appeared possibly 1100 BC • Origin was probably from closely related animal pox viruses of the orthopox virus group • Smallpox became worldwide and endemic throughout Europe and caused pandemics with high mortalities in the Americas • Responsible for estimated 300 million deaths in 20th century
Control of Smallpox • Variolation developed in Far East and introduced to Europe • 1796: First vaccinia-based vaccination by Edward Jenner • 1967: Enhanced WHO eradication program • 1972: Vaccination ended in US • 1977: Last natural case of smallpox (Somalia) • 1978: Last death/case of smallpox, lab acquired – air vent system, Janet Parker in Birmingham, England • 1980: WHO declared smallpox eradicated • 1984: Official repositories of variola designated as CDC in Atlanta, GA and Vector in Novosibirsk, Russia
Smallpox – Current Concerns • Soviet government bioweapons program • Aimed to produce smallpox in large quantities and adapt it for use in bombs and ICBMs • Industrial capacity capable of producing many tons of smallpox virus annually • Stocks in official repositories may not be secure • With break-up of Soviet Union, security at Vector was poor • Risk that rogue states did not destroy stocks • Could be used for bioterrorism purposes
History of Vaccinia as Smallpox Vaccine • Vaccinia obtained from animals, presumably cows or horses • Member of Orthopox family • Related to both cowpox and variola • Initially propagated from person to person • The coordinated use of two standardized vaccinia strains, Lister and NYCBH, were responsible for eradicating smallpox worldwide by 1980
Evidence of Protection • Cutaneous Reaction (dermal take) • “Major reaction” correlates with • Protection against smallpox • Development or presence of neutralizing antibodies and T cells • Neutralizing Antibodies • Neutralizing antibodies correlate with protection against smallpox in humans • Mice and monkeys with neutralizing antibodies and T cell depletion are protected • Passive immunization provides some protection • T cells may also play an important role
Protection from Vaccination • Complete protection for three to five years • Partial protection for up to 25 years • Perhaps long-term protection against death Fenner F et al. Smallpox and its Eradication, pp53
Historic Understanding of Adverse Events: Data from US Routine Vaccination Programs in 1960s
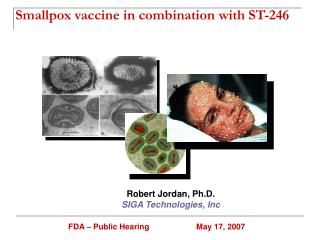
Progression of Smallpox Source: CDC
Clinical Features of Smallpox • Discrete • Confluent • Flat • Hemorrhagic
Areas of normal skin between pustules even on face Smallpox – Discrete Source: CDC
Confluent rash on face and forearms Smallpox – Confluent Source: CDC
Pustules confluent or semiconfluent – appear flat Smallpox – Flat Source: CDC
Widespread hemorrhage into skin, early and late forms, 98% case fatality Smallpox – Hemorrhagic Source: CDC
Smallpox Mortality Mortality from infection with variola major in unvaccinated individuals can be up to 50%
Conclusions • Smallpox is a devastating disease with a very high mortality rate in the non-immune • Vaccination historically associated with significant adverse events • Populations are immunologically vulnerable following eradication and end of vaccination programs • In the United States, few people have been vaccinated in 34 years Continued
Conclusions (Continued) • As long as variola virus exists anywhere, there will be the need to have a smallpox vaccine available in the event of a bioterrorism threat or laboratory accident • It is in our best interest to have a modern smallpox vaccine available
ACAM2000 Smallpox Vaccine Development Program Thomas P. Monath, MD Former Acambis Chief Scientific Officer
Vaccine Development Goals Met • Purified clone derived from Dryvax®(NYCBH vaccinia strain) • Well characterized seed lot free of adventitious agents • GMP manufacturing in cell culture (Vero) using modern standards • Meets all release specifications including potency ≥ 108 PFU/mL • Clinical safety similar to or better than Dryvax® • Demonstrated clinical efficacy (some differences from Dryvax®)
Indication/Use • Vaccination with ACAM2000 is indicated for protection of persons determined to be at high risk for smallpox infection • Not for routine vaccination of general population • Stored and controlled by Strategic National Stockpile (SNS)
Topics to be Covered • Introduction • Nonclinical data • Clinical data • Safety • Efficacy • Conclusions
Nonclinical Summary • Toxicology studies in mice and cynomolgus macaques inoculated IC show ACAM2000 less neurovirulent than Dryvax® • ACAM2000 and Dryvax® have similar immunogenicity in mice and monkeys • Both vaccines protect mice and cynomolgus macaques against lethal homologous and heterologous poxvirus challenge
ACAM2000 Is Less Neurovirulent than Dryvax®3-4 Day-old Mice Inoculated IC, n=32/Group
ACAM2000 and Dryvax® Elicit Similar Immune Responses and Protect Cynomolgus Monkeys against Lethal Monkeypox Challenge (3.8 x 107 PFU IV)
Topics to be Covered • Introduction • Nonclinical data • Clinical data • Safety • Efficacy • Conclusions
Subjects Evaluated for Safety * Phase III study enrollment curtailed due to myocarditis AEs. Planned enrollment 2040 ACAM2000 and 680 Dryvax®
Common Adverse Events • Expected AEs known to be associated with smallpox vaccinations • Inoculation site reactions, lymphadenitis, feverishness, chills, fatigue, malaise, myalgia • The incidence of these AEs was higher for Dryvax® than ACAM2000
Solicited Adverse Events Occurring in ≥10% of Subjects by Treatment Group, Phase III
Myocarditis • Prospective case ascertainment Phase I (H-400-002) and Phase III • ECGs at screening, Day 10 and 21 (Phase III) or screening and Day 15 (Phase I) • Troponin I and/or CK-MB at screening and Day 10 (Phase III) or Day 15 (Phase I) • Provoked cardiac AEs (clinic visits, diaries) • Myocarditis seen only in vaccinia-naïve subjects • Previous under-reporting based on passive surveillance and symptomatic cases only
Myocarditis – Phase I (H-400-002) and Phase III (Vaccinia-naïve Subjects, Standardized Case Ascertainment)
Topics to be Covered • Introduction • Nonclinical data • Clinical data • Safety • Efficacy • Conclusions
Vaccine Efficacy • Efficacy cannot be demonstrated in disease setting due to eradication of smallpox • Cutaneous Response is a generally accepted surrogate of protection (WHO, ACIP) • Neutralizing Antibodies are a correlate of protection • May be more accurate reflection of vaccine effectiveness in previously vaccinated subjects with modified ‘takes’ • Historical data suggest relatively low titers are protective • Mack et al., 1972 (protective titer >1:32) • Sarkar et al., 1975 (protective titer >1:20)