Download
1 / 40
490 likes | 944 Vues
Chapter 13: Anxiety Disorder: Phobia. Unit 4 – AOS 2 Mental Health Pages 630-673. Anxiety and Anxiety Disorders. • application of a biopsychosocial framework to understanding and managing simple phobia as an example of an anxiety disorder:

E N D
Chapter 13: Anxiety Disorder: Phobia Unit 4 – AOS 2 Mental Health Pages 630-673
Anxiety and Anxiety Disorders • application of a biopsychosocial framework to understanding and managing simple phobia as an example of an anxiety disorder: – biological contributing factors: role of the stress response; role of the neurotransmitter gamma-amino butyric acid (GABA) in the management of phobic anxiety – psychological contributing factors: psychodynamic, behavioural and cognitive models; the use of psychotherapies in treatment including cognitive behavioural therapy (CBT), systematic desensitisation and flooding – socio-cultural contributing factors: specific environmental triggers such as being bitten by a dog; parental modelling and transmission of threat information – the interaction between biological, psychological and socio-cultural factors which contribute to an understanding of the disorder and its management
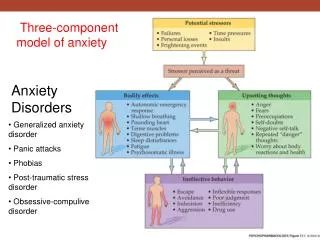
Anxiety and Anxiety Disorders • Anxiety is a state of physiological arousal associated with feelings of apprehension, worry or uneasiness that something is wrong or that something unpleasant is about to happen • It is normal to experience anxiety in certain situations but it should be brief and temporary – if anxiety is severe or exaggerated and does not subside, it can be counterproductive and disabling • Experiencing severe anxiety can indicate the presence of an anxiety disorder – the term anxiety disorder is used to describe a group of disorders that are characterised by chronic feelings of anxiety, stress, nervousness and apprehension or fear about the future, with a negative effect
Phobias • We all have fears but they are not necessarily severe enough to interfere with out daily lives • A phobia is an excessive or unreasonable fear directed towards a particular object, situation or event that causes significant distress or interferes with everyday functioning • It is estimated that phobias affect approx. 3% of the Australian population with more females than males affected
Specific Phobia • A specific phobia is a disorder characterised by significant anxiety provoked by exposure to a specific feared object or situation, often leading to avoidance behaviour
Specific Phobia • According to the DSM-IV-TR, any specific phobia falls into one of five categories • 1. of animals (eg. birds, spiders, insects) • 2. of situations (eg. lifts, bridges, enclosed spaces) • 3. of blood, injections and injury (eg. seeing blood, watching surgery) • 4. of the environment (eg. lightning, darkness, heights) • 5. other phobias • Traditionally specific phobias are names using Greek prefixes that stand for the object or situation (arachnophobia – fear of spiders, claustrophobia – fear or enclosed spaces) • All phobias share common symptoms but primarily differ in that they occur in response to specific objects or situations
Specific Phobia • Earlier versions of the DSM used the term ‘simple phobia’ to describe a phobia but specific phobia is now used because a specific object or situation is the focus of the fear • When someone is exposed to the phobic stimulus, an anxiety response is triggered, similar to a stress response – in some cases this can be so intense it takes the form of a panic attack (the onset of intense anxiety that can last for a few minutes up to an hour or so) • Box 13.2 – Panic attack, pg. 637 • People with a specific phobia are aware their fear is excessive and unreasonable and may often feel embarrassed because of their fear • They can often feel compelled to avoid the phobic stimulus and can begin to organise their life around this avoidance
Specific Phobia • Anticipatory anxiety is the gradual rise in anxiety levels as the person thinks about or anticipates being exposed to the phobic stimulus in the future • As with all disorders in the DSM-IV-TR, the persons anxiety, avoidance behaviours or anticipatory anxiety significantly interferes with their everyday lives and/or causes them great distress – a diagnosis can only be made if this has persisted for a period of at least 6 months • Learning Activity 13.1 – Review questions, pg. 637
Biological Contributing Factors • Many research studies on the biological factors that contribute to specific phobias and other types of anxiety disorders have investigated whether some people may be more genetically predisposed than others to specific fears and high anxiety levels – these studies indicate that we may inherit a predisposition to develop an anxiety disorder • Other biological factors involved in specific phobias are the role of the stress response and the role of the brains neurotransmitters, specifically GABA
Role of the Stress Response • Phobic anxiety becomes a problem when the stress response is triggered in the absence of any real threat or danger • For people with a specific phobia, their stress response is triggered by exposure, or anticipated exposure, to objects or situations which are perceived to be dangerous • Anxiety is therefore problematic for someone with a specific phobia as their anxiety tends to excessive as their perception of threat is unreasonable and out of proportion with what it should be – this means that the stress response they experience is often very sever and can persist at this high level for longer
Role of GABA • GABA and glutamate are naturally occurring neurotransmitters that carry messages between neurons in the brain • Gamma-amino butyric acid (GABA)is the primary inhibitory neurotransmitter in the CNS and works throughout the brain to make postsynaptic (receiving) neurons less likely to fire • Without the inhibitory effects of GABA, neurons in the brain may fire out of control causing seizures such as in epilipsy • Glutamate is the primary excitory neurotransmitter in the CNS, making postsynaptic neurons more likely to fire • The two act to counter the effects of each other and play a big role in regulating CNS arousal
Role of GABA • GABA is believed to play a role in anxiety • Benzodiazepines are a group of drugs (commonly known as tranquillizers) which have the effect of ‘calming’ the body down by reducing physiological arousal and promoting relaxation • These drugs work by imitating and therefore stimulating a neurotransmitters activity (agonist) or by inhibiting a neurotransmitters activity (antagonists) • Benzodiazepines are GABA agonists – they imitate GABA and stimulate activity at the site of the postsynaptic neuron where GABA is received from a presynaptic neuron • Box 13.3 – Benzodiazepines, pg. 641
Role of GABA • Studies have shown the benzodiazepines are effective in the management of specific phobias (for example, someone with a fear of flying may be prescribed to take valium before boarding the plane to reduce their anxiety to a tolerable level) • Ethyl alcohol has a similar effect on GABA receptors • The connection between the level of GABA in the brain and anxiety symptoms have led researchers to hypothesis that some people develop anxiety due to having a dysfunctional GABA system • The level of GABA in the brain can be affected by a variety of things such as genetic inheritance, prolonged stress or exposure to toxic chemicals
Role of GABA • Some have proposed that GABA can be increased naturally by drinking green tea or eating foods high in GABA, as well as using GABA supplements • There is no significant evidence however that GABA supplements can penetrate the blood-brain barrier which is physiological mechanism that protects the brain and spinal cord from undesirable toxins in the blood
Psychological Contributing Factors • Although finding the origin of a specific phobia is sometimes difficult, a number of models have been devised to describe and explain how a specific phobia can develop due to psychological factors • These include the psychodynamic model, the behavioural model, and the cognitive model
Psychodynamic Model • The psychodynamic model was proposed in the late 1800’s by Freud and is based on an assumption that all mental disorders are caused by unresolved psychological conflicts that occur in the unconscious part of the mind, beneath the level of ordinary conscious awareness • These conflicts have their origins in early childhood experiences, during which our instinctive impulses and society’s view of what is ‘acceptable’ behaviour often clash • According to Freud, the unconscious part of our mind is a storage place for all the information which is not acceptable to the conscious mind
Psychodynamic Model • Freud also proposed that following birth we progress through a series of five psychosexual stages • Oral stage (0-2 years) • Anal stage (2-3 years) • Phallic stage (4-5 years) • Latency stage (6 years-puberty) • Genital stage (Puberty-early adulthood) • In defining these stages Freud used the term ‘sex’ very loosely to refer to something that was physically pleasurable rather than something specifically sexual • In each stage different parts of the body become the focus of attention and pleasure for the individual, in addition, each stage has a crucial developmental conflict that must be satisfactory resolved in order to move to the next stage – if not resolved it can be the source of anxiety
Psychodynamic Model • Usually we protect ourselves against anxiety by using defence mechanisms which Freud described the unconscious process by which the conscious part of our mind (termed the ‘ego’) defends or protects itself against anxiety arising from unresolved internal conflicts • According to Freud, a specific phobia develops as a consequence of an unresolved Oedipal complex • This Oedipal complex, as described by Freud, is a developmental conflict that emerges during the phallic (third) stage of psychosexual development and describes the unconscious, powerful, passionate love and desire that a male child has developed towards his mother • This term is used now to describe the desire of either a male or female child to ‘possess’ the opposite-sex parent and ‘eliminate’ the same-sex parent
Psychodynamic Model • Freud described this desire as unconscious because the boy is not ‘consciously aware’ of it; soon after developing their desire, the boy begins to fear that his father, who is bigger and more powerful than he is, will become aware of his son’s desire for his mother and punish him • According to Freud, in order to successfully resolve the Oedipal complex, the male child uses the defence mechanism known as repression to prevent the socially unacceptable desire for his mother, and the anxiety accompanying this desire, from entering conscious awareness • When repression does not work, another type of defence mechanism called displacement will be used
Psychodynamic Model • Displacement involves directing feelings away from the object or person that causes them to a substitute object that is less threatening • This means that the anxiety caused by the unresolved Oedipal complex is redirected onto another seemingly unimportant object or situation which then becomes the phobic stimulus • Freud (1909) first explained his ideas about how specific phobias developed in a case study called ‘Analysis of a phobia in a five-year old boy’ (pg. 644-645)
Behavioural Model • According to the behavioural model, phobias are learned through experience and may be acquired, maintained or modified by environmental consequences such as rewards or punishment • These models are based on learning theories by Skinner, Watson and Pavlov • Watson’s ‘Little Albert’ experiment was the first to demonstrate that specific phobias can be acquired through classical conditioning
Behavioural Model • After acquisition due to classical conditioning, a specific phobia is typically maintained through operant conditioning although operant conditioning can also contribute to the acquisition of a phobia • An example of this is where parents may unintentionally provide reinforcement for a child's initial fear of a particular stimulus
Cognitive Model • In explaining how a specific phobia may be acquired and persist, a cognitive phobia focuses on how the individual processes information about the phobic stimulus and related events • For example, explanations of phobias from a cognitive perspective tend to examine how people with phobias tend to think about a phobic stimulus and its context, and their perceptions, memories, beliefs, attitudes, bias, appraisals, expectations and other cognitive processes that may be relevant • A key assumption of many cognitive models is that people with a specific phobia often have one or more cognitive biases • A cognitive bias is a tendency to think in a way that involves errors of judgement and faulty decision-making; essentially a cognitive bias involves a ‘mistake in thinking’
Attentional Bias • Attentional bias is the tendency to selectively attend to threat-related stimuli rather than neutral stimuli • Someone with a specific phobia may tend to pay greater attention to threatening information while ignoring non-threatening information • People with phobias tend to be hypervigilant – that is they are always alert and constantly looking around for something relevant to their phobia • A person with a phobia of horses may notice a horse walking towards them but fail to pay attention to the farmer walking behind the horse with Memory Bias • In relation to phobias memory bias occurs when recall or recognition is better for negative or threatening information than for positive or neutral information • A person with a phobia of horses will tend to remember the time they were chased by a horse but will not recall all of the other times when they were not
Interpretive Bias • In relation to phobias, interpretive bias (also called judgemental bias) is the tendency to interpret and judge ambiguous stimuli and situations in a threatening manner • A person with a phobia of spiders may interpret a piece of black fluff on the floor to be a spider Catastrophic Thinking • Catastrophic thinking is a type of negative thinking in which an object or event is far more threatening, dangerous or insufferable than it really is and will result in the worst possible outcome
Socio-cultural Contributing Factors • Many socio-cultural factors may contribute to an individual developing a phobia • Three of the most common are • Specific environmental triggers • Parental modelling and; • Transmission of threat information
Specific Environmental Triggers • Many people with a specific phobia report having a negative or traumatic experience with a particular phobic stimulus at some time in the past • These ‘specific’ objects or situations in the ‘environment’ produced or ‘triggered’ an extreme fear response at the time, hence the name specific environmental triggers • Often an initial fear response becomes a conditioned fear response through classical conditioning processes • Research indicates that the more severe the trauma associated with an unpleasant or harmful fear experience, the more likely it is that a phobia will develop
Parental Modelling • Observational learning, or modelling, can also be involved in the development of a phobia – a child who observes a parent react with sheer panic to the sight of a spider or mouse may imitate the same behavioural response • Children are most vulnerable to developing specific phobias via parental modelling as they do not have knowledge or experience or know whether or not their parents behaviour is appropriate or rational • Parents can help prevent excessive fears developing in their children by modelling ‘bravery’ or other positive methods for coping with fear
Transmission of Threat Information • Most people who have fear of flying have never been in a plane crash – yet this is one of the most common phobias • Transmission of threat information refers to the delivery of information from parents, other family members, peers, teachers, the media and other secondary sources about the potential threat or actual danger of a particular object or situation • Box 13.7 – Transmission of threat information by movies, pg. 653 • Learning Activity 13.6 – Summarising socio-cultural factors, pg. 655
Psychological Management of Specific Phobias • For some people, phobias can cause major disruptions to their lives if the phobic stimulus is continually experienced or if the person goes to major lengths to avoid the stimulus • People typically only seek help in the form of therapy if the phobic stimulus is frequently encountered or can’t be avoided • Some of the therapies available include; • Cognitive behavioural therapy (CBT) • Systematic desensitisation, and • Flooding
Cognitive Behavioural Therapy (CBT) • CBT (as we have seen) combines cognitive and behavioural therapies to try and help people manage mental health problems and disorders • Cognitive therapy is a type of ‘talking therapy’ that focuses on the role of cognitions in determining emotions and behaviour • Behavioural therapy is the clinical application of learning theories, such as those described by Skinner. Pavlov and Watson • While cognitive therapy deals with maladaptive thoughts and beliefs, behavioural therapy deals directly with maladaptive behaviours such as avoidance and reduced anxiety levels, which can maintain or worsen a person’s psychological problems and the thoughts and feelings associated with them
Cognitive Behavioural Therapy (CBT) • When using CBT, the emphasis on the cognitive or the behavioural component can vary, depending on the disorder and the symptoms the person reports • CBT aims to assist the person to identify where they may have become trapped or stuck in their way of thinking and to assist them to learn and use other ways of thinking about their situation • When using CBT, it is important that, from the outset, the mental health professional clearly explains to their client the difference between thoughts, feelings and behaviour and their interrelationship
CBT for Specific Phobias • In addressing the thoughts underlying a specific phobia, the cognitive component of CBT aims to assist the client to develop a new understanding that the feared stimuli is not dangerous, so their avoidance and safety behaviours are unnecessary • When using CBT, mental health professionals encourage their client to first identify their fear and anxiety related thoughts and their cognitive biases, as these strongly affect whether someone will experience fear and anxiety when exposed to a phobic stimulus • The client is then encouraged to look for evidence that supports their fear cognitions and evidence that does not support them – sometimes a persons cognitive distortions arise from a lack of information or inaccurate information
CBT for Specific Phobias • Once a person has identified their cognitive distortions, they are more likely to counter them with alternative, more objective, and useful thoughts • Engaging in more balanced and objective thinking about their phobic stimulus will then lead to changes in their feelings and behaviours, particularly a reduction in fear, anxiety and avoidance • The behavioural component of CBT aims to change any behaviours that are maladaptive – one way a mental health professional using CBT may attempt to reduce or eliminate their clients maladaptive behaviours is by encouraging them to engage in one or more behavioural experiments
CBT for Specific Phobias • Behavioural experiments are planned experiential activities that are undertaken by clients in or between CBT sessions • The main purpose is to help the client ‘test out’ the accuracy of their cognitive distortions • The steps to set up a behavioural experiment are similar to those used to carry out scientific research • Make a prediction • Review existing evidence for and against the prediction • Devise a specific experiment to test the validity of the prediction • Note the results • Draw conclusions • The behavioural component of CBT may also make use of systematic desensitisation and flooding
Systematic Desensitisation • Systematic desensitisation is a kind of behaviour therapy that aims to replace an anxiety response with a relaxation response when an individual with a specific phobia confronts a fear stimulus • This type of therapy applies classical conditioning principles in a process that involves unlearning the connection between anxiety and a specific object or situation and reassociating feelings of relaxation and safety with that particular object or situation
Systematic Desensitisation • Strategies may include progressive muscle relaxation, visual imagery or the slow breathing technique (SBT) • An anxiety or fear heirachy or produced, ranking approximations of the anxiety or fear producing stimulus into a sequence ranging from most fear producing to least fear producing – most consist of 10-15 specific situations which is rated on a 100 point scale • These situations are then paired with relaxation techniques and worked up the heirachy which can be achieved by real life or visual imagery
Flooding • Flooding is similar to systematic desensitisation but does not have a relaxation component to help combat anxiety – when used for treating phobias, flooding involves bringing the client into direct contact with their most feared object and situation straight away and keeping them in contact with it until their fear and anxiety disappear • The underlying principle is that anxiety will be experienced at a very high level and then gradually diminish • Like systematic desensitisation, flooding can be conducted in vivo, through the use of visual imagery or by using a virtual reality device • Unlike systematic desensitisation, flooding is used to deliberately produce a massive fear response • Learning Activity 13.11 – Review questions, pg, 667