Download
1 / 36
430 likes | 1.12k Vues
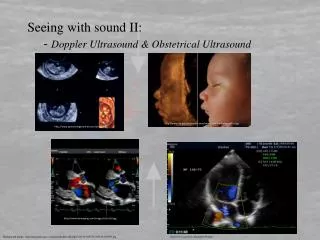
DOPPLER ULTRASOUND in Pregnancy. Dr. Mohammed Abdalla Egypt, Domiat Hospital. Doppler History. First use of Doppler ultrasonography to study flow velocity in the fetal umbilical artery was reported in 1977. Doppler History. Fitzgerald & Drumm. Umbilical artery studies 1977 BMJ

E N D
DOPPLER ULTRASOUND in Pregnancy Dr. Mohammed AbdallaEgypt, Domiat Hospital
Doppler History First use of Doppler ultrasonography to study flow velocity in the fetal umbilical artery was reported in 1977
Doppler History • Fitzgerald & Drumm. Umbilical artery studies 1977BMJ • Eik-Nes et al. Fetal aortic velocimetry : Dupplexscanner 1980 Lancet • Campbell et al. Utero-placental circulation: Dupplex scanner 1983 Lancet • Wladimiroff et al. MCA / UA PI ratio 1987 OG • Kiserud et al. Ductus venosus velocimetry 1991Lancet
Echoes from stationary tissues are the same from pulse to pulse. Echoes from moving objects exhibit slight differences in the time for the signal to be returned to the receiver. These differences can measured as phase shift from which the Doppler frequency is obtained. . Basic principals
T1 : time of omitted signal . T2 : time of returned signal . T2 – T1 = time difference or phase shift . from phase shift the Doppler frequency is obtained. AS TIME DIFFERENCE DECREASE THE DOPPLER FREQUENCY INCREASE.
T2 T1 pulse repetition frequency (T2 –T1) phase shift with known beam / flow angle can calculate flow velocity .
The time difference or phase shift are then proceeded to produce either colorflow display or a Doppler sonogram Basic Principals
Basic Principals • ‘Doppler frequency’ is obtained by measuring the time difference for the signal to be returned when reflected from moving scatterers . • Doppler frequency increase if: • flow velocity increased . • beam is more aligned to the direction of flow. • higher transducer frequency is used.
Factors affecting doppler frequency Freq. 3 (the angle q between the beam and the direction of flow becomes smaller). This is of the utmost importance in the use of Doppler ultrasound. 2 The angle of insonation q Flow velocity 1
(the angle q between the beam and the direction of flow becomes smaller). This is of the utmost importance in the use of Doppler ultrasound. beam(A) is more aligned than (B) The beam/flow angle at (C) is almost 90° and there is a very poor Doppler signal The flow at (D) is away from the beam and there is a negative signal.
Aliasing If a second pulse is sent before the first is received, the receiver cannot discriminate between the reflected signal from both pulses and aliasing occur.
Aliasing So to eliminate aliasing The pulse repetition frequency or scale is set appropriately for the flow velocities
Basic Principals The volume flow in the UAs increases with advancing gestation. The high vascular impedance detected in the first trimester gradually decreases. It is attributed to growth of placental unit and increase in the number of the functioning vascular channels.
Uses • plays a vital role in the diagnosis of fetal cardiac defects . • assessment of the hemodynamic responses to fetal hypoxia and anemia. • diagnosis of other non-cardiac malformations.
Anatomy • Blood supply provided by the ovarian and uterine arteries • Uterine Arteries: main branches of the internal iliac arteries • Uterine Arteries: Ascend through the lateral wall and anastomose with the ovarian arteries
Anatomy • Arcuate Arteries: Run Circumferentially around the uterus • Uterus: Blood supply to anterior and posterior walls provided by the Arcuate arteries • Radial Arteries: Extend from the arcuate arteries and enter the endometrium • Spiral Arteries: connect the maternal circulation to the endometrium • Responsible for a 10 fold increase in blood flow
Anatomy • Conversion of small muscular spiral arteries into large vascular channels transforms the uteroplacental circulation into a low-resistance-to-flow system. These have a dilated and tortuous lumen, a complete absence of muscular and elastic tissue, no continuous endothelial lining.
Umbilical artery UMBILICAL ARTERY FLOW characteristic saw-tooth appearanceof arterial flow in one direction and continuous umbilical venous blood flow in the other.
FACTORS AFFECTING UMBILICAL ARTERY DOPPLER FLOW VELOCITY WAVEFORMS*
Umbilical artery Benefit of Umbilical Artery Evaluation Less experienced operators can achieve highly reproducible results with simple, inexpensive continuous-wave equipment .
The 40% of the combined fetal ventricular output is directed to the placenta by two umbilical arteries. The assessment of umbilical blood flow provides information on blood perfusion of the fetoplacental unit . . Umbilical artery
Umbilical artery • With advancing gestation, umbilical arterial Doppler waveforms demonstrate a progressive rise in the end-diastolic velocity and a decrease in the pulsatility index.
The possible Doppler velocimetry sites Middle cerebral artery Using color flow imaging, the middle cerebral artery can be seen as a major lateral branch of the circle of Willis, running anterolaterally at the borderline between the anterior and the middle cerebral fossae
Middle cerebral artery The blood velocity increases with advancing gestation, and this increase is significantly associated with the decrease in PI
Middle cerebral artery An early stage in fetal adaptation to hypoxemia - central redistribution of blood flow ( brain-sparing reflex) increased blood flow to protect the brain, heart, and adrenals reduced flow to the peripheral and placental circulations
Doppler wave form of early stage offetal hypoxemia increased end-diastolic flow in the middle cerebral artery (lower MCA pulsatility index or resistance index) Average of both MCAs must be calculated for more precise result
Middle Cerebral Artery Flow velocity waveform in the fetal middle cerebral artery in a severely anemic fetus at 22 weeks (left) and in a normal fetus (right). In fetal anemia, blood velocity is increased
Middle Cerebral Artery When the fetus is hypoxic, the cerebra arteries tend to become dilated in order to preserve the blood flow to the brain and The systolic to diastolic (A/B) ratio will decrease (due to an increase in diastolic flow)
Doppler ultrasound for the fetal assessment in high-risk pregnancies (Cochrane Review). In: The Cochrane Library, 1999. Neilson JP and Alfirevic Z • Trudinger et al 1987 • McParland et al 1988 • Tyrrell et al 1990 • Hofmeyr et al 1991 • Newham et al 1991 • Burke et al 1992 11 Studies Included In Analysis Almstrom et al 1992 Biljan et al 1992 Johnstone et al 1993 Pattison et al 1994 Nienhuis et al 1997
Doppler ultrasound for the fetal assessment in high-risk pregnancies • Nearly 7000 patients were included • The trials compared no Doppler ultrasound to Doppler ultrasound in high-risk pregnancy (hypertension or presumed impaired fetal growth) Meta analysis
Doppler ultrasound for the fetal assessment in high-risk pregnancies Main results • A reduction in perinatal deaths. • Fewer inductions of labour . • Fewer admissions to hospital . • no report of adverse effects . • No difference was found for fetal distress in labour . • No difference in caesarean delivery .
Biophysical profile for fetal assessment inhigh risk pregnancies • When compared with conventional fetal monitoring (usually cardiotocography) biophysical profile testing showed no obvious effect (either beneficial or deleterious) on pregnancy outcome. There was an increase in the number of inductions of labour following biophysical profile in the trial. Alfirevic Z, Neilson JP. Biophysical profile for fetal assessment in high risk pregnancies (CochraneReview). In: The Cochrane Library, 1995.