Download
1 / 1
10 likes | 125 Vues
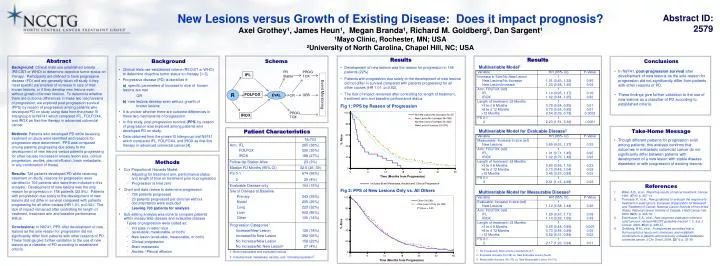
New Lesions versus Growth of Existing Disease: Does it impact prognosis? Axel Grothey¹, James Heun¹, Megan Branda¹, Richard M. Goldberg², Dan Sargent¹ ¹Mayo Clinic, Rochester, MN; USA ²University of North Carolina, Chapel Hill, NC; USA. Abstract ID: 2579. Results Multivariable Model 1

E N D
New Lesions versus Growth of Existing Disease: Does it impact prognosis? Axel Grothey¹, James Heun¹, Megan Branda¹, Richard M. Goldberg², Dan Sargent¹ ¹Mayo Clinic, Rochester, MN; USA ²University of North Carolina, Chapel Hill, NC; USA Abstract ID: 2579 Results Multivariable Model1 Multivariable Model for Evaluable Disease2 Multivariable Model for Measurable Disease3 Abstract Background: Clinical trials use established criteria (RECIST or WHO) to determine objective tumor status on therapy. Participants are defined to have progressive disease (PD) and are generally taken off study if they meet specific parameters of increase in size of their known lesions, or if they develop new lesions even without growth of known lesions. To determine whether there are outcome differences in these two mechanisms of progression, we explored post-progression survival (PPS) by reason of progression among patients who developed PD on study using data from the phase III Intergroup trial N9741 which compared IFL, FOLFOX4, and IROX as first-line therapy in advanced colorectal cancer. Methods: Patients who developed PD while receiving treatment on study were identified and reasons for progression were determined. PPS was compared among patients progressing due solely to the development of new lesions versus patients progressing for other causes (increase in known lesion size, clinical progression, ascites, pleural effusion, brain metastasis, or any combination of these). Results: 726 patients developed PD while receiving treatment on study; reasons for progression were identified in 703 patients who were then included in this analysis. Development of new lesions was the only reason for progression in 158 patients (22.5%). Patients with progression due solely to the development of new lesions did not differ in survival compared with patients progressing for all other causes (HR 1.01, p=0.92). The lack of impact remained after controlling for length of treatment, treatment arm and baseline performance status. Conclusions: In N9741, PPS after development of new lesions as the sole reason for progression did not significantly differ from patients with other reasons of PD. These findings give further validation to the use of new lesions as a classifier of PD according to established criteria. • Results • Development of new lesions was the reason for progression in 158 patients (22%) • Patients with progression due solely to the development of new lesions did not differ in survival compared with patients progressing for all other causes (HR 1.01, p=0.92). • The lack of impact remained after controlling for length of treatment, treatment arm and baseline performance status. • Fig 1: PPS by Reason of Progression • Fig 2: PPS of New Lesions Only vs. All Others Background Conclusions Schema • Clinical trials use established criteria (RECIST or WHO) to determine objective tumor status on therapy [1-3]. • Progressive disease (PD) is identified if: • a) specific parameters of increase in size of known lesions are met • OR • b) new lesions develop even without growth of known lesions • It is unclear whether there are outcome differences in these two mechanisms of progression. • In this study, post-progression survival (PPS) by reason of progression was explored among patients who developed PD on study. • Data obtained from the phase III Intergroup trial N9741 which compared IFL, FOLFOX4, and IROX as first-line therapy in advanced colorectal cancer [4]. • In N9741, post-progression survival after development of new lesions as the sole reason for progression did not significantly differ from patients with other reasons of PD. • These findings give further validation to the use of new lesions as a classifier of PD according to established criteria. PR Stable PROG TOX IFL R EVAL FOLFOX Event Monitoring OBS CR PROG TOX IROX • Take-Home Message • Though different patterns for progression exist among patients, this analysis confirms that outcomes in metastatic colorectal cancer do not significantly differ between patients with development of a new lesion with stable disease elsewhere or with progression of existing lesions. Patient Characteristics • Methods • Cox Proportional Hazards Model: • Adjusting for treatment arm, performance status and length of time on treatment prior to progression • Progression is time zero • Chart and data review to determine progression • 726 patients progressed • 23 patients progressed per clinician without documentation were excluded • Leaving 703 patients for analysis • Sub-setting analysis was done to compare patients within measurable disease and evaluable disease • Types of progression were coded as: • Increase in lesion size (evaluable, measurable, or both) • New lesion (evaluable, measurable, or both) • Clinical progression • Brain metastasis • Ascites / Pleural effusion Includes Brain Metastasis, Ascites and ‘Clinical Progression • References • Miller, A.B., et al., Reporting results of cancer treatment. Cancer, 1981. 47(1): p. 207-14. • Therasse, P., et al., New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst, 2000. 92(3): p. 205-16. • Eisenhauer, E.A., et al., New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer, 2009. 45(2): p. 228-47. • Goldberg, R.M., et al., A randomized controlled trial of fluorouracil plus leucovorin, irinotecan, and oxaliplatin combinations in patients with previously untreated metastatic colorectal cancer. J Clin Oncol, 2004. 22(1): p. 23-30. 1 - No Increase/No New Lesions excluded (N=27) 2 - Evaluable Increase (N=138) vs. New Evaluable Lesion (N=44) 3 - Measurable Increase (N=175) vs. New Measurable Lesion (N=112) 1- Both measurable and evaluable lesions 2- Includes brain metastasis, ascites, and “clinical progression”