Download
1 / 44
450 likes | 593 Vues
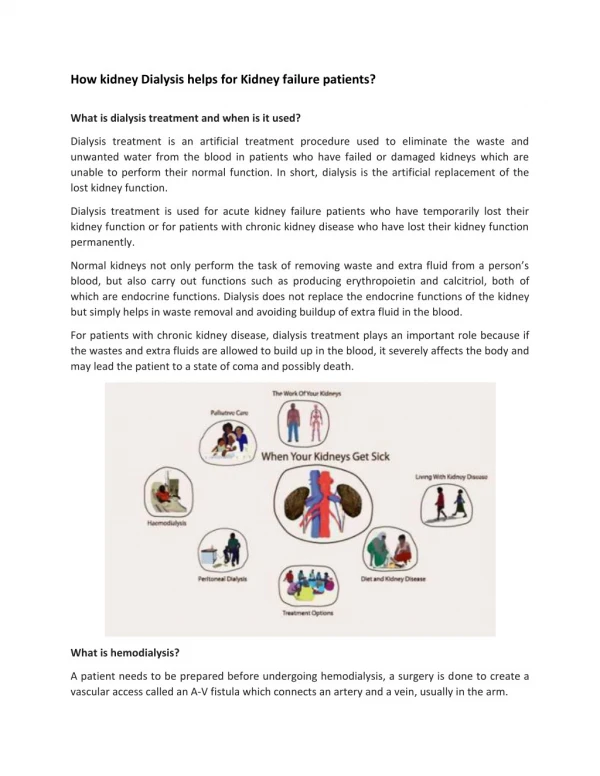
Nutrition for Patients with Kidney Disorders Chapter 21. Nutrition for Patients With Kidney Disorders. Kidneys perform many vital functions Urinary excretion is the primary method by which the body rids itself of: Excess water & Toxic substances Nitrogenous wastes & Organic acids

E N D
Nutrition for Patients With Kidney Disorders • Kidneys perform many vital functions • Urinary excretion is the primary method by which the body rids itself of: • Excess water & Toxic substances • Nitrogenous wastes & Organic acids • Electrolytes & Drugs • Sulfates
Nutrition for Patients With Kidney Disorders (cont’d) • The kidneys help to regulate acid–base balance by secreting hydrogen ions to increase pH and excreting bicarbonate to lower pH • Involved in blood pressure regulation • Play an important role in maintaining normal metabolism of calcium and phosphorus • Kidney diseases can profoundly impact metabolism, nutritional status, and nutritional requirements
Nephrotic Syndrome • A generic term that refers to a kidney disorder characterized by urinary protein losses greater than 3.0 g/d • Major symptoms: • Proteinuria • Hypoalbuminemia • Hyperlipidemia • Edema
Nephrotic Syndrome (cont‘d) • Hypoalbuminemia and proteinuria • May lead to protein calorie malnutrition, anemia, increased risk of infection, vitamin D deficiency, and increased clotting • Hyperlipidemia increases the risk of cardiovascular disease and progressive renal damage • Causes of nephrotic syndrome include diabetes, autoimmune diseases (e.g., lupus, IgA nephropathy), infection, and certain chemicals and medications
Nephrotic Syndrome (cont’d) • In some cases, treating the underlying disorder corrects nephrotic syndrome • In others cases, especially diabetes, nephrotic syndrome may be the beginning of chronic kidney disease
Nephrotic Syndrome (cont’d) • Nutrition therapy • Goals • To minimize edema, proteinuria, and hyperlipidemia • To replace nutrients lost in the urine • To reduce the risk of progressive renal damage and atherosclerosis
Nephrotic Syndrome (cont’d) • Nutrition therapy (cont’d) • Benefits of minimizing proteinuria • An increase in serum albumin, a decrease in serum lipid levels, a slower progression of kidney disease, and less edema
Nephrotic Syndrome (cont’d) • Sodium and fluid • Sodium restriction begins when fluid retention occurs • For stages 1 to 4 and hemodialysis: • 1,000 to 3,000 mg/day are recommended • Range is 2,000 to 4,000 mg for peritoneal dialysis
Nephrotic Syndrome (cont’d) • Sodium and fluid • Fluid is unrestricted in stages 1 to 4 with normal urine output • For people on hemodialysis, fluid allowance equals the volume of any urine produced plus 1,000 mL
Nephrotic Syndrome (cont’d) • Phosphorus and calcium • As kidney function deteriorates, the conversion of vitamin D to its active form is impaired • National Kidney Foundation recommends both phosphorus and calcium intake be controlled
Nephrotic Syndrome (cont’d) • Phosphorus and calcium • In stages 1 to 4, phosphorus allowance is based on lab values and calcium is limited to 1000 to 1,500 mg/day • Phosphate binders must be taken with all meals and snacks
Question • Nephrotic syndrome can be caused by what? a. Lupus b. Proteinuria c. Stress d. Hyperlipidemia
Answer a. Lupus Rationale: Causes of nephrotic syndrome include diabetes, autoimmune diseases (e.g., lupus, IgA nephropathy), infection, and certain chemicals and medications.
Chronic Kidney Disease (CKD) • A syndrome of progressive kidney damage and loss of function • Decrease in the number of functioning nephrons overburdens the remaining nephrons, and the kidney’s ability to filter blood deteriorates • Measured by a decrease in glomerular filtration rate (GFR)
Chronic Kidney Disease (CKD) (cont’d) • The impact on nutrition • Loss of kidney function produces widespread effects • As urine output decreases, fluid and electrolytes accumulate in the blood, producing symptoms of overhydration such as increased blood pressure, weight gain, edema, shortness of breath, and lung crackles
Chronic Kidney Disease (CKD) (cont’d) • The impact on nutrition • Uremic syndrome (uremia) is a serious complication of CKD and acute renal failure. It occurs when urea and other waste products build up in the body because the kidneys are unable to eliminate them. These substances can become poisonous (toxic) to the body if they reach high levels. Text p. 517
Chronic Kidney Disease (CKD) (cont’d) • The impact on nutrition • Acidosis occurs because the kidneys are unable to excrete acid produced through normal metabolic processes
Chronic Kidney Disease (CKD) (cont’d) • CKD is associated with premature mortality and decreased quality of life • Progresses slowly and may not be apparent until 50% to 70% of function is lost • In stages 1 to 4, medical and nutrition therapy can potentially delay the progression to stage 5
Chronic Kidney Disease (CKD) (cont’d) • Modifiable risk factors • Smoking cessation, an increase in physical activity, and controlling blood lipid levels • Stage 5 requires dialysis or kidney transplant for survival • Diabetes is the leading cause of CKD • Other risk factors include cardiovascular disease, hypertension, and obesity
Chronic Kidney Disease (CKD) (cont’d) • The impact on nutrition • Reabsorption of some nutrients is impaired • GI absorption of some minerals, such as calcium and iron, is impaired
Chronic Kidney Disease (CKD) (cont’d) • The impact on nutrition • Impaired synthesis of rennin, erythropoietin, and the active form of vitamin D can lead to high blood pressure, anemia, and bone demineralization • Accelerated atherosclerosis increases the risk of coronary heart disease, myocardial infarction, and further renal damage
Nutrition therapy • Goals • Reduce workload on the kidneys • Restore or maintain optimal nutritional status • Control the accumulation of uremic toxins • Diet modifications are made in response to symptoms and laboratory values and require frequent monitoring and adjustment • Diet is both complex and dynamic
Nutrition therapy (cont’d) • Protein • As kidney function declines, the ability to excrete nitrogenous and other wastes also declines • Modification of Diet in Renal Disease (MDRD) study showed that tight control of blood pressure and a restricted protein intake of 0.6 g/kg/day helped delay the progression of kidney disease by 41%
Nutrition therapy (cont’d) • Protein (cont’d) • In stages 1 to 4, the recommended daily protein intake is 0.6 g/kg to 0.75 g/kg • Protein allowance may be liberalized to maintain appropriate body protein stores or because the severity of restriction is too difficult to follow • Protein allowance in stage 5 is 50% higher than the RDA to account for the loss of serum proteins and amino acids in the dialysate
Nutrition therapy (cont’d) • Calories • When protein intake is restricted, it is vital to consume adequate calories to spare protein from being used for energy, enabling it to be used for protein synthesis • For all stages of CKD: • Calorie recommendations are 35 cal/kg for adults under 60 years of age • 30 to 35 cal/kg for those who are older
Nutrition therapy (cont’d) • Calories (cont’d) • During peritoneal dialysis, a large amount of calories is absorbed daily through the dialysate (approximately 340 to 680 cal/day) • Calories from the dialysate impair the natural sense of hunger and generally prevent a fall in blood glucose levels between meals • Increased intake of pure sugars and pure fats helps to meet calorie requirements while keeping protein intake low
Nutrition therapy (cont’d) • Sodium and fluid (cont’d) • Intake is monitored by weight gain • For many clients on hemodialysis, fluid restriction is hardest
Nutrition therapy (cont’d) • Potassium • Loss of kidney function means potassium excretion is impaired and hyperkalemia is a risk • Hypokalemia is a risk for people who receive continuous ambulatory peritoneal dialysis, take potassium-wasting diuretics, or who experience vomiting or diarrhea • At all CKD stages, potassium allowance is based on the individual’s serum potassium levels
Nutrition therapy (cont’d) • Other vitamins and minerals • Specially formulated vitamin supplements • Deficiencies of water-soluble vitamins • Fat-soluble vitamins A and E have been shown to accumulate in CKD • Clients who are undergoing dialysis may develop a deficiency of zinc • IV iron for clients receiving hemodialysis
Translating recommendations into meals • Diet for CKD is complex • “Choice” system, similar to the diabetic exchange system, may be used to help clients implement dietary restrictions • Individualized meal plan • Selections can be severely limited
Diabetic kidney disease • Formerly known as diabetic nephropathy • Risk factors for diabetic kidney disease (DKD) • Hyperglycemia, hypertension, and altered lipid levels • Nutrition therapy seeks to controls these risks
Question • What are the calorie recommendations for patients with chronic kidney disease? a. 40 cal/kg for adults under 60 years; 35 to 40 cal/kg for those who are older b. 35 to 40 cal/kg for all adults c. 35 to 40 cal/kg for adults under 60 years; 30 to 35 cal/kg for those who are older d. 35 cal/kg for adults under 60 years; 30 cal/kg for those who are older
Answer d. 35 cal/kg for adults under 60 years; 30 cal/kg for those who are older Rationale: Calorie recommendations are: 35 cal/kg for adults under 60 years of age; 30 to 35 cal/kg for those who are older
Nutrition Recommendation Guidelines for Diabetic Kidney Disease • Protein 0.8 g/kg • Sodium 2,300 mg/d • Lipids ≤30% calories from fat, <10% calories from saturated fat, 200 mg cholesterol/d • Carbohydrates 50% to 60% of total calories • Phosphorus 1,700 mg/d for stages 1 and 2 • 800 to 1000 mg/d for stages 3 and 4 • Potassium <4,000 mg/d for stages 1 and 2 • 2,400 mg/d for stages 3 and 4
Chronic Kidney Disease (CKD) (cont’d) • Kidney transplantation • A treatment option for people with stage 5 CKD • Immediate postoperative diet is high in protein and calories to promote healing • Most dietary parameters are removed when the new kidney functions normally • Lifelong commitment to “healthy” eating is important
Acute Renal Failure • Acute renal failure (ARF) is the sudden loss of renal function characterized by an acute increase in serum creatinine and decrease in urine output • Can develop over a period of hours or days • Can range from mild to severe • Causes: shock, severe infection, trauma, medications, and obstruction • Primary focus of treatment is to correct the underlying disorder
Acute Renal Failure (cont’d) • Nutrition therapy • It has not been proven that nutrition therapy for ARF promotes recovery of kidney function or improves survival • Goal is to provide adequate amounts of calories, protein, and other nutrients to prevent or minimize malnutrition • It is difficult to achieve nutritional goals with oral, enteral, or parenteral nutrition
Acute Renal Failure (cont’d) • Nutrition therapy (cont’d) • One approach is to strictly limit fluid, electrolytes, and protein • For patients who are malnourished and hypercatabolic, the approach may be to give ample amounts of protein and nutrients and provide dialysis as needed • Oral, enteral, or parenteral nutrition is given
Kidney Stones • Form when insoluble crystals precipitate out of urine • 75% of kidney stones are made of calcium oxalate • Risk factors: • Dehydration or low urine volume, urinary tract obstruction, gout, chronic inflammation of the bowel, and intestinal bypass or ostomy surgery • High fluid intake dilutes the urine
Kidney Stones (cont’d) • Oxalate • Normally only 6% to 14% consumed is absorbed • Calcium • Binds with dietary oxalate in the intestines, forming an insoluble compound that the body cannot absorb • Protein • High intakes of animal protein increase urinary excretion of calcium, oxalate, and uric acid and reduce urinary pH • Sodium • A high sodium intake promotes urinary calcium excretion by decreasing calcium reabsorption by the kidneys
Kidney Stones (cont’d) • Nutrition therapy • None of the diet recommendations made to prevent kidney stones are effective when used alone
Question • Is the following statement true or false? The goal of nutrition therapy for acute renal failure (ARF) is to provide an adequate amount of calories, protein, and other nutrients to prevent or minimize malnutrition. This is easy to achieve with either oral, enteral, or parenteral nutrition.
Answer False. Rationale: Goal is to provide adequate amounts of calories, protein, and other nutrients to prevent or minimize malnutrition. It is difficult to achieve nutritional goals with oral, enteral or parenteral nutrition.