Download
1 / 33
330 likes | 485 Vues
Risk Factors for Smoking in the EMR Region Kawkab Shishani, BSN, PhD The Hashemite University Epidemiology of Diabetes & Other Non-Communicable Diseases Alexandria, Egypt 6-13 th January 2009. Petra: Jordan’s Wonder of the World. Objectives. Describe the scope of the problem

E N D
Risk Factors for Smoking in the EMR Region Kawkab Shishani, BSN, PhD The Hashemite UniversityEpidemiology of Diabetes & Other Non-Communicable DiseasesAlexandria, Egypt6-13th January 2009
Objectives • Describe the scope of the problem • Examine smoking among selected populations • Differentiate between forms of tobacco use • Discuss why smoking is harmful • Value WHO position on tobacco control • Summarize how health care professionals can provide the leadership in tobacco control
Question Why it is important to study smoking ? • Smoking is the chief avoidable risk factor for NCDs • Smoking Affects the progression of NCDs (> complications) • Unlike the other risk factors such as physical activity and nutrition that affects only those who do not comply to them, smoking affects smoker as well as those around
Why Do Farmers Grow Tobacco? The wealth generated by leaf tobacco production helps to improve quality of life and attracts educational, health and social facilities in, otherwise, relatively impoverished, rural areas. International tobacco growers association http://www.tobaccoleaf.org/about_itga/index.asp?op=1
Scope of the Problem • 1,3 billion smokers: • 80% in developing countries • 20% in developed countries • The number is expected to increase by 1.7 per cent annually • By 2030, 80% of deaths due to tobacco will occur in developing countries
Scope of the Problem • Most cigarettes consumed worldwide are international brands • As smoking rates in the US and Europe is declining, new markets are needed • Globalization made it easy for companies to access new markets internationally (Asia, Africa, Middle East)
Smoking: Men and Women • Global smoking (M: 4> F) • ↑ in smoking rates in F > M • Ratio of smoking M: F • Developed countries 3:1 • Developing countries 7:1
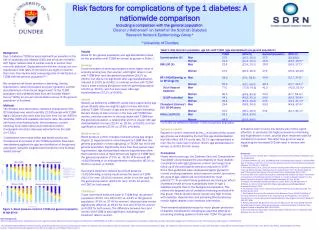
Smoking: Men and Women EMR country profilehttp://www.emro.who.int/TFI/CountryProfile
Smoking: Men and Women • 50%-66% of women use “light” • Addiction in M>F • Biological responses to nicotine differ between M & F • Smoking in women is reinforced by less nicotine than in men (Perkins et al., 1991)
Female Smoking & Low Birth Weight www.globalheathfactt.org
Smoking: Youth WHO (2007). Sifting the evidence: Gender and tobacco control
Youth Smoking in EMR EMR country profilehttp://www.emro.who.int/TFI/CountryProfile
I can't stop smoking. I am addicted to cigarettes. Smoking: Youth • Parent (father smokes) • Access to cigarettes • Peer pressure • Experimentation • Imitating adults
Forms Of Tobacco Use • Waterpipe • Cigarettes • Chewing
Second Hand Smoking • At home: • Smoking around children • Children prepare waterpipe for parents • Cultural issues • Public places (hospitals, buses, taxis,..)
Waterpipe: The Emerging Epidemic • Myths: • It is safe alternative for cigarettes (WHO study group , 2005) • Chemicals filtered by the water (bubbling) • Not addictive; can quit anytime (Asfar et al. BMC Public Health 2005) • Highest rates are in MENA (Shihadeh., 2004) • Social practice (Café employees) • Children smoke with their parents (Maziak et al., 2004)
Waterpipe: The Emerging Epidemic • Nicotine in 1 head of unflavored tobacco = 70 regular cigarettes; • Flavored tobacco = 20cigarettes • A single smoking session: 2.25 mg nicotine, high levels of arsenic, cobalt, chromium, and lead (Shihadeh, 2003) • Cotinine levels are almost the same among waterpipe and cigarette smokers (Bacha, Salameh, Waked , 2007)
Chemicals Produced From Smoking • Nicotine • Tar • Carbon monoxide • Benzopyrene • Cyanide hydrogen
How Does Nicotine Work? From Benowitz N. Nicotine Addiction. Primary Care 1999; 26(3):611-31
Why Nicotine Matters Short term effect Long term effect
Tobacco Dependence: A Chronic Disease • The long delay between the onset of smoking and associated morbidities • 70% of the smokers want to quit Unsuccessful • 44% tried to quit • Only 7% succeed
Tobacco Dependence: A Chronic Disease • A Chronic disease model: • Long term nature • Minimum number achieve permanent abstinence • Periods of relapse and remissions • No ideal intervention • Emphasis on education and counseling (same like in DM, HTN) (US Department of Health and Human Services, 2008)
WHO Efforts to Control Tobacco Use (FCTC) • Price and tax measures • Protection from exposure to tobacco smoke • Educational and public awareness programmes • Promoting the cessation of tobacco use • Sales to and by minors • Research, surveillance and exchange
Where Do We Go From Here? Monitoring tobacco use to provide accurate tracking of epidemiological data about the extent of tobacco exposure (GTSS) Report morbidities associated with smoking Public Education (media, curricula) Health Insurance companies (reimburse tobacco dependence treatments)
Why Do We Need A Plan in EMR Lack of human resources (experienced in tobacco control Lack of adequate studies on hazards of smoking Research encouragement (Funding) http://www.emro.who.int/tfi/CountryProfile-Part6.
5 As A1. Ask—Systematically identify all tobacco users at every visit A2. Advise—Strongly urge all tobacco users to quit A3. Assess—Determine willingness to make a quit attempt A4. Assist—Aid the patient in quitting (provide counseling and medication) A5. Arrange—Ensure follow-up contact Treating Tobacco Use and Dependence: 2008 Update” Clinical Guideline
Elements of Counseling Problem solving/ skills training Recognize danger situations – Develop coping skills- Identify and practice coping Provide basic information Supportive treatment Encourage the patient in the quit Attempt Communicate caring and concern. Encourage the patient to talk about the quitting process. Treating Tobacco Use and Dependence: 2008 Update” Clinical Guideline
Format of Counseling Assessment Program clinician Program intensity Format Type of counseling Medication Population Treating Tobacco Use and Dependence: 2008 Update” Clinical Guideline