Download

1 / 38
500 likes | 1.01k Vues
Mycobacterium tuberculosis. A Brief History. What is Mycobacterium tuberculosis ?. The causative agent of tuberculosis, aka TB, aka Consumption, aka White Death Mycobacterium tuberculosis is part of the M. tuberculosis complex.

E N D
Mycobacterium tuberculosis A Brief History
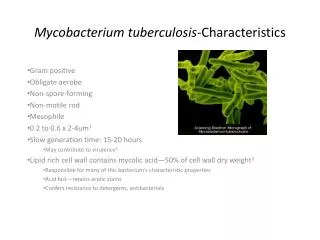
What is Mycobacterium tuberculosis? • The causative agent of tuberculosis, aka TB, aka Consumption, aka White Death • Mycobacterium tuberculosis is part of the M. tuberculosis complex. • On the basis of growth rate, catalase and niacin production, and pigmentation in light or dark, Mycobacteria are classified into members of the Mycobacterium tuberculosis complex (M. tuberculosis, M. bovis, M. africanum, M. microtii) and non-tuberculous species. Gene probe technology now facilitates this distinction. • Although not considered to be gram-stainable, it is a weakly gram-positive rod • It is an acid-fast, non-motile, non-spore-forming, pleomorphic slender rod and an obligate aerobe. • It is slow growing (3-8 weeks or 12-24 hours doubling time) • It is fastidious, growing only on Lowenstein-Jensen and Middlebrook. • Althoughthere areother species causing TB, this is the only causative agent of human TB.
Culture Media • Lowenstein-Jensen • Relatively inexpensive at ~$3 per tube/plate • The original formulation of Lowenstein-Jensen media was developed by Lowenstein who incorporated Congo red and malachite green to inhibit unwanted bacteria. The present formulation is based upon Jensen’s modification. Jensen’s version eliminates Congo red and uses a moderate concentration of malachite green to preventgrowth of the majority of contaminants surviving decontamination of the specimen. This formulation also encourages the earliest possible growth of Mycobacteria. • Fresh eggs are added aseptically to this media. During heating, the egg albumin coagulates, thus providing a solid surface for inoculation. Nitrogen, fatty acids, and proteins are suppliedby egg and asparagine. Glycerol serves as a carbon source and is favorableto the growth of the human type tubercle bacillus while being unfavorableto the bovine type. Malachite green acts as an inhibitory agent towards microorganisms other than Mycobacteria.
Culture Media con’t • Middlebrook 7H10 • Over the years, many culture media have been devised for the cultivation of Mycobacteria. The early ones were egg-based formulations and included Lowenstein-Jensen Medium. Dubos and Middlebrook were instrumental in the development of a numberof formulations which contained oleic acid and albumin as key ingredients to aid in the growthof the tubercle bacilli and to protect the organisms against a variety of toxic agents. Subsequently,Middlebrook and Cohn improved the formulation of oleic acid-albumin agar and obtained faster, more luxuriant growth ofMycobacterium species on their medium designated as 7H10.It has been reported that the 7H10 medium tends to grow fewer contaminants than the egg-basedmedia commonly used for the cultivation of Mycobacteria. • Contains human blood and is used for the isolation and cultivation of Mycobacterium spp. This medium contains a variety of inorganic salts, sodium citrate, vitamins, cofactors, oleic acid, albumin, biotin, catalase and glycerol. Sodium citrate when converted to citric acid, holds the inorganic cations in solution. Glycerol is provided as an abundant source of carbon and energy for the tubercle organisms. Malachite green is added as a selective agent, which partially inhibits the growth of other bacteria. Biotin and catalase help stimulate the revival of the damaged organism. OADC Enrichment contains the following required additives: albumin to protect the tubercle bacilli against toxic agents, oleic acid, a fatty acid utilized in the metabolism of the organism; sodium chloride to maintain osmotic equilibrium, catalase to destroy any toxic peroxides in the medium, and dextrose as an energy source. • The 10% human blood provides necessary components that promote the growth of M. genavense. The human blood components which promote growth of the organism have not yet been identified. • Inexpensive (roughly $1.25 per tube/plate)
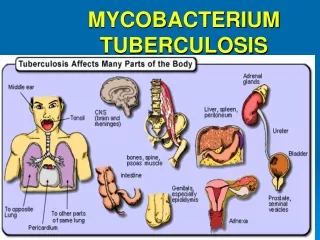
The Disease • Tuberculosis grows intracellularly in alveolar macrophages. • The disease is primarily due to the host response macrophages which clump together in giant cells called Langhans cells. • They are then spread in the blood to other organs. • In other words, it grows in the very cells that are supposed to kill it!
Symptoms • Granulomas keep the infection from advancing until immunity is decreased. • Fever, weakness, cough with bloody sputum • Infects the upper lobes of the lungs. • Causes necrosis in the tissues.
Treatment and Prevention • Tx: Multiple drug regimen for ~9 mos. • There are drug resistant strains. • Prevention: Prophylaxis of multiple drug regimen for 6-12 mos. with suspected TB exposure. • BCG vaccine • Wear PPE when there is a possibility of being exposed.
Historical Reference • TB has infected the human population for thousands of years. • Fragments from the spinal columns of Egyptian mummies dating back to 2400 BCE have been found to show pathological signs of tubercular decay. • A recent study genetically typed M. tuberculosis as a young strain. It is not known which strain of Mycobacterium came first. • More research is necessary to determine if the multiple strains are due to cattle to human transmission or due to the nomadic lifestyles of the humans which brought them into closer contact with multiple races of people.
Sylvius • In 1679, he wrote his Opera Medica in which he described actual tubercles as a characteristic change in the lungs and other parts of the body in consumptive patients. • He went on to describe the abscessesand cavities that followed.
Benjamin Marten • An English physician who theorized that TB could be caused by “wonderfully minute living creatures”. • He also thought that a healthy person could catch the disease if they spent a large amount of time in contact with an infected person, but the disease was rarely transmitted with short periods of contact. • “It may be therefore very likely that by an habitual lying in the same bed with a consumptive patient, constantly eating and drinking with him, or by very frequently conversing so nearly as to draw in part of the breath he emits from the Lungs, a consumption may be caught by a sound person…I imagine that slightly conversing with consumptive patients is seldom or never sufficient to catch the disease.”
Hermann Brehmer • In 1854, suffering from TB, he was sent to live in the Himalayas on advice from his physician. After returning home cured, he began to study medicine and presented his doctoral dissertation bearing the auspicious title, Tuberculosis is a Curable Disease. • He built the first sanitorium.
Important Advancements • 1865 – Jean-Antoine Villemin demonstrated that TB could be passed between species. He postulated that the disease was caused by a specific microorganism and did not arise spontaneously as was previously thought. • 1882 – TB was first viewed when Robert Koch discovered a special staining technique that allowed him to view the microorganism.
1895 – Wilhelm Konrad bon Rontgen discovered a radiation that could be used to view the progress and severity of a patient’s disease. • A further development was the BCGT vaccine, which is still used today. Calmette and Guerin were able to lower the virulence of the bovine strain of TB which lead to the creation of the vaccine. • 1943 – Selman A. Waksman was successful in finding an antibiotic that worked against TB infection. Streptomycin was first administered to a human on November 20, 1944. • Progression of the disease immediately halted. • The bacteria disappeared from the sputum. • The patient recovered fully. • Other drug therapies and combinations soon followed.
Further Developments • 1946 – Para-aminosalisylic acid (PAS) found to be moderately effective against TB. • 1947 – TB shows resistance to Streptomycin • 1948 – Streptomycin and PAS used effectively together against TB. • 1951 – new drug – Isoniazid (INH) created. Shown to be more effective with PAS than Streptomycin. • 1954 – the drug pyrazinamide is created • 1955 – the drug cycloserene is produced. • 1962 – Ethambutol is created. • 1963 – Rifampicin is used to treat TB. • 1980’s – New drug resistant strains surfaced, threatening vulnerable groups such as the urban poor and the immunocompromised.
Phlebotomy: the ancient art of bloodletting. • The practice of bloodletting seemed logical when the foundation of all medical treatment was based on the four body humors: blood, phlegm, yellow bile, and black bile. Health was thought to be restored by purging, starving, vomiting or bloodletting. • The art of bloodletting was flourishing well before Hippocrates in the fifth century B.C. By the middle ages, both surgeons and barbers were specializing in this bloody practice. Barbers advertised with a red (for blood) and white (for tourniquet) striped pole. The pole itself represented the stick squeezed by the patient to dilate the veins. • Bloodletting came to the U. S. On the Mayflower. The practice reached unbelievable heights in the 18th and early 19th centuries. The first U.S. President, George Washington, died from a throat infection in 1799 after being drained of nine pints of blood within 24 hours. The draining of 16-30 ounces (one to four pints) of blood was typical. Blood was often caught in a shallow bowl. When the patient became faint, the "treatment" was stopped. Bleeding was often encouraged over large areas of the body by multiple incisions. By the end of the 19th century (1875-1900), phlebotomy was declared quackery.
A sanatorium patient receives pneumothorax treatment from Dr. GH Hames in Saskatchewan during the 1940s. Pneumothorax Therapy Lung Collapse Therapy
Artificial pneumothorax includes the compression of the diseased lung. The pleural cavities were filled with gas or filtered air, which was repeated daily, with a gradual decrease of treatments. The treatments would be continued sporadically for up to two to four years after the initial treatment. • Bilateral pneumothorax included the compression of both lungs. Only parts of the lungs were collapsed so that patients could still live relatively normal lives. The patients suffered from shortness of breath caused by the decreased lung space.
Thoracoplasty • This method was more extreme than the previous two. Ribs from one side of the thorax were removed in order to collapse the infected portion of the lung permanently.
Gold Therapy Holger Mollgaard, in Copenhagen first put this type of treatment to use in 1925. He introduced the compound sanocrysin, which is a double thiosulfate of gold and sodium. He tested the compound on animals and deemed it safe to use on humans. However, despite claims to the contrary by physicians Secher and Faber, it was wholly toxic. Danish and British physicians began using smaller doses to combat tuberculosis. Despite smaller doses, it still remained toxic. A test trial was completed in America and proved the toxic effects of gold therapy in 1934. Within a year, most of Europe had ceased to use gold therapy. Gold Deposits Secondary to Gold Therapy
Sanatoriums There were many sanatoriums created in the 20th century for the treatment and isolation of TB patients. Initially, there were very few spaces available and they were only open to the elite. They were often well-maintained and provided rest, fresh air, good food, and a “great mindset” for the patients. By 1950, there were hundreds of thousands of beds available across the United States alone. With the creations of streptomycin and isoniazid in the 1940s, many of the sanatoriums were phased out of use. They were converted to hospitals, religious facilities, and convalescent homes. Several sanatoriums had attained negative reputations and were claimed to be haunted and were considered full of “germs”. These institutions remained empty for many years following the closure of the sanitorium.
Special Happenings in the TB Community • There were special radio stations devoted to airtime for TB patients in TB Hospitals. The patients or their family and friends could call in requests and send messages to each other over the radio. • In Canada, thousands of Indigenous Inuit people were removed from their villages and taken south for treatment, never to be heard from again. There is a huge effort on the part of Social Services and the Inuit peoples to uncover lost records to help the families reunite or to find the remains of their loved ones who died and were buried without the knowledge of their families.
Why were non-white people more susceptible to Mycobacterium tuberculosis? • They weren’t!
It was widely believed that non-white people were more susceptible to TB due to their color of skin. • Non-white people were living in poverty. • They were largely uninformed due to illiteracy. • Non-white people had no access to proper healthcare. • Many hospitals only admitted white people. • Unlike the U.S., Canada treated everyone regardless of race, sex or ability to pay.
How is TB treated today? • One of the most important parts of today’s response to TB is in the testing process. We now have tried and proven ways of testing for the disease with known processes for definitive identification.
After the Diagnosis • Following the definitive diagnosis of TB, there are many ways to treat and cure TB. • There are many drugs and combinations of drugs that can be used depending on the sensitivity of the strain. • The outcome of the treatment depends on compliance of the patient.
Is TB still a problem today? • YES!!!
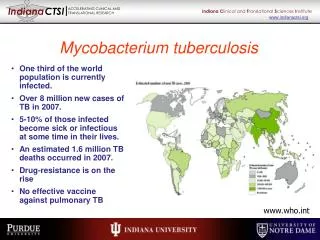
TB kills nearly 3 million people per year! • Nearly one-third of the world’s population is infected with TB. • TB causes more deaths than any other infectious agent in the world. • Despite all the drugs available today, TB is still a problem in developing nations. • The highest incidences are in countries in Africa, Asia, and Latin America. • The World Health Organization estimates that each year, 3 million people die from TB, and 8 million more people are infected.
TB is found in many workplaces in the United States. • Healthcare facilities • Correctional Institutions • Homeless shelters • Long-term care facilities for the elderly • Drug treatment centers
Why is TB on the rise? • Homelessness • Intravenous drug usage • Overcrowding in institutional settings • HIV infection • Drug resistant strains of TB • Reduced TB control and treatment sources • Immigration from high TB prevalence areas • In the 1980’s, AIDS created a community that was susceptible to the disease of TB.