Download
1 / 30
300 likes | 422 Vues
THE EBOLA VIRUS EPIDEMIC Current S tatus and Future Prospects. William Schaffner, MD Professor of Preventive Medicine and Infectious Diseases Vanderbilt University Medical Center Consultant, Communicable Disease Control Tennessee Department of Health. OUTLINE.

E N D
THE EBOLA VIRUS EPIDEMIC Current Status and Future Prospects William Schaffner, MD Professor of Preventive Medicine and Infectious Diseases Vanderbilt University Medical Center Consultant, Communicable Disease Control Tennessee Department of Health
OUTLINE Ebolavirus ecology and epidemiology Ebolavirus disease – clinical aspects Public Health Response Research: Treatment and Vaccines Ebola in the USA
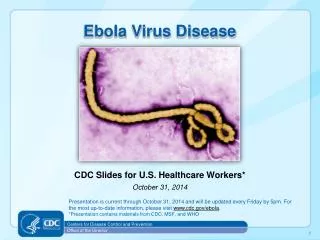
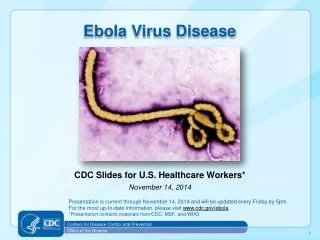
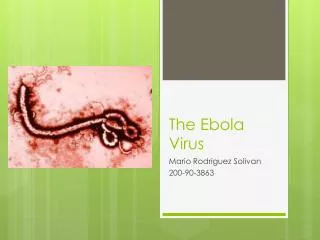
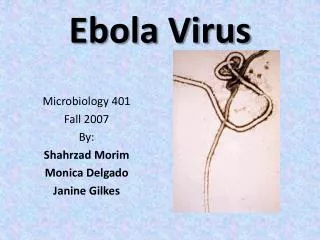
Filovirus family (filo, Latin for filament) Hemorrhagic Fever Viruses Five subtypes West African epidemic: Zaire subtype
Ebolavirus Ecology • Likely reservoir: Fruit bats • Large, roost in large colonies, migrate • Infected hosts: Great apes, forest antelopes Humans likely infected via hunting/butchering animals Perhaps contact with bat urine, droppings or saliva on partially eaten fruit
EBOLA CLINICAL ASPECTS - 1 Incubation period 5-10 Days (range, 2-19) ONSET: Abrupt – Fever, Headache, Myalgia Soon Thereafter: Nausea, Vomiting, Abdominal Pain, Diarrhea Ongoing: Jaundice, Pancreatitis CNS – Somnolence, Delirium, Coma Bleeding (1/3) – Petechiae, Hemorrhages
EBOLA CLINICAL ASPECTS - 2 Electrolyte abnormalities – sodium and potassium loss Liver failure → low serum protein → edema Bleeding from low platelets Fatality rate, current outbreak: ~50%
Human – to – Human Transmission Patients become infectious to others when they become sick Ebolavirus is NOT spread by respiratory route Spread from intimate contact with body fluids or tissues of a sick person or a corpse
Two Primary Risk Groups for Transmission • Healthcare workers: all who touch patients, soiled environment, funeral/burial workers • Family members • Caring for the sick • Preparation of loved one’s body for burial cultural bathing, touching of respect
2 y.o. boy Gueckedou, Guinea Intersection of 3 nations Dec, 2013 1 week Mother, sister, grandmother Mourners to another village Health worker another village Relatives other towns doctor Relatives other towns Mar, 2014 Ebola recognized Dozens Dead in 8 Guinean towns Suspected cases in Liberia, Sierra Leone Funeral of traditional healer 14 women infected Koindu, Sierra Leone
MOLECULAR GENETIC STUDY OF THE WEST AFRICAN EBOLA VIRUS Investigators: Harvard, Broad Institute, Kenema Hospital in Sierra Leone Sequenced RNA, 99 virus samples All the viruses are closely related-traced back to single introduction by traditional healer Outbreak NOT caused by repeated introductions from nature: all human-to-human spread
Contributions to Rapid Spread - 1 • Previous outbreaks in small, remote villages • Current: A border region, more dense population Roads improved, people travel a lot • West Africa had not experienced Ebola before • Economy poor, low education, recent political instability • Rumors that Ebola was a myth or a political fiction
Contributions to Rapid Spread - 2 • Limited healthcare facilities, few healthcare personnel poorly trained, no personal protective supplies • Abandonment of healthcare facilities • Facilities refuse to treat anyone with suggestive symptoms • Families keep ill at home and keep quiet to avoid stigma
HEALTHCARE LIMITATIONS “Beds” may be pallets on the floor or ground Facilities often do not provide support services Families prepare food for patient Hygienic care by family Facilities may not have capacity to do CBCs, electrolytes, other blood tests Some do not have running water
RESPONSE • Treatment of the sick • Humanitarian and public health goals • Rigorous surveillance • How many ill, ages, where located • Contact tracing, quarantine and observation • Education/Community engagement • Disposal of the dead • NOT cordon sanitaire
RESPONSE LIMITATIONS • Country governments poor, lack public health infrastructure, slow sense of responsibility • Doctors Without Boarders (MSF) cried an alarm, but without a response • WHO suffered budget cuts – its epidemic response unit profoundly diminished
INTERNATIONAL RESOURCES Personnel: Clinical, public health Administrative, logistical WHO, NGOs, CDC, Faith-based Personal Protective Equipment Masks, gloves, impervious gowns, etc., etc. Equipment for clinical care labs, beds, IV fluids, etc., etc.
TREATMENT RESEARCH ZMAPP. Molecular biologic production of 3 antibodies against Ebola SHOWN TO WORK IN EXPERIMENTAL INFECTIONS In monkeys: all 18 who got 3 infusions survived 3 untreated died NOT yet shown to work in humans
VACCINE RESEARCH • GSK/NIH Chimpanzee adenovirus vector that expresses Zaire and Sudan glycoprotein Phase I trial started • Public Health Agency of Canada/NIH/Walter Reed Vesicular stomatitis recombinant vaccine Phase I trial soon
Please Remember – this is Research Experimental: No proven therapeutic or preventive effect Safety in humans: Unknown If something works: Implementation research Ethical, cross-cultural issues No magic bullets
WILL EBOLA COME HERE? Virus has been in labs here for years High profile patients (Kent Brantly, Nancy Writebol, Rick Sacra) Ebola candidate patients – show up at Hospital X Ebola will NOT establish itself in the US
HOSPITALS CAN CARE FOR EBOLA PATIENTS SAFELY Isolation room Personal Protective Equipment with Sentinal Environmental, Waste Disposal, Lab Safety Mock patient drills, Education
SAFE HOSPITAL CARE STAT contact with Tennessee Department of Health Communication and education Media relations Would be intense
EBOLA IN WEST AFRICANEAR-TERM FUTURE Grim Predictions up to 20,000+ cases Many Months Concern for spread to other West African countries Food supplies Transport Economic/Political destabilization
USA EBOLA INFLUENZA Old – annual Conventional Known Often deadly 5-20% infected annually 200,000 hospitalized ~32,000 deaths Wash hands Avoid coughers Get vaccinated! New Mysterious Unknown Deadly 0 infected 3 hospitalized 0 deaths No sense of personal control