Download
1 / 62
620 likes | 630 Vues
Thyroid Diseases West China Hospital of Sichuan Univesity Sichuan University, West China School of Medicine Department of Internal Medicine Division of Endocrinology and Metabolism Wangqin ( 王覃 ), MD. Part 1 Classification of Thyroid Diseases.

E N D
Thyroid Diseases West China Hospital of Sichuan Univesity Sichuan University, West China School of Medicine Department of Internal Medicine Division of Endocrinology and Metabolism Wangqin (王覃), MD
Part 1 Classification of Thyroid Diseases • Congenital: Enzyme deficiency, abnormal development (structure, location, morphology), pregnant woman(gestational)- associated....... • Clinical manifestation: overt subclinical 3. Function: Hyperfuntion- thyrotoxicosis ≠ hyperthyroidism Hypofunction- hypothyroidism
Part 1 Classification of Thyroid Diseases 4. Morphology and structure: enlargement (goiter) atrophy mass or nudule 5. Localization: ectopic 6. Pathogenesis: autoimmune- AITD non-autoimmune- non-AITD
Part 1 Classification of Thyroid Diseases • Diseases: A.Thyroiditis- fulminant acute: infection, radiation subacute: pain (granulomatous) painless(lymphocytic) chronic: Hashimoto (chronic lymphocytic) Riedel(fibrotic)
Part 1 Classification of Thyroid Diseases 7. Diseases: B. simple goiter C. Graves disease(thyroiditis?) D. tumor E. ectopic F. tuberculosis G. trauma and injury
Part 1 Classification of Thyroid Diseases 8. Iatrogenic 9. Factitious 10.others: A. abnormal metabolism of thyroid hormones (euthyroid sickness syndrome, non- thyroid illness syndrome……) B. thyroid hormone resistance(T3-R ß mutation) C. TSH resistance D. TSH gene mutation E. TSH-R gene mutation … …
What is thyrotoxicosis? A clinical condition or syndrome encompassing several specific diseases, clinically characterized by hypermetabolism, and biochemically elevated or inappropriate high serum levels of free thyroid hormones and their action in tissue, includes hyperthyroidism as one cause.
Task1 • 请根据甲状腺素的生理功能,推理甲状腺素过多和过少会产生什么样的临床表现(时间10分钟,讨论5分钟+参观5分钟) • 形式:分4-6组讨论,选择一名同学为秘书做记录。将讨论结果(要求以短语形式)写在一张A3大小的纸上面(分成两半,一半甲亢一半甲减),然后按照顺时针顺序进行换组参观,参观时需要把补充或不同的意见以不同颜色的笔标记在纸上(尽量以生动模式进行,比如画画)
Symptoms and Signs of thyrotoxicosis Nervousness and irritability (99%) Heat intolerance and increased sweating (90%) Increased resting heart rate causing palpitations (90~100%) Atrial fibrillation(10%) Tremor (97%) (hypersympathicotonus) Fatigue(88%) Embolic event(rare)
Symptoms and Signsthyrotoxicosis Weight loss (85%)or alterations in appetite(65%) Frequent bowel movements (23%) Thyroid enlargement (goiter) Sudden paralysis
Symptoms and Signsthyrotoxicosis Thin, delicate skin and irregular fingernail Menstrual disturbance (decreased flow) Impaired fertility Mental disturbances Sleep disturbances (including insomnia)
Symptoms and Signsthyrotoxicosis Older patients may present atypically with apathetic or masked hyperthyroidism. The circulatory manifestations may predominate, while the nervous manifestations are lacking or minimal. Orbitopathy is less common in elderly patients, who are more likely to develop muscular weakness, prostration, anorexia
Thyroidhormone/functiondetermine • TSH • T3 • T4 • FT3 • FT4 • rT3
Thyroidantibodies • Thyroglobulin (Tg, formerly known as the colloid antigen) • Thyroid peroxidase (TPO, formerly known as the microsomal antigen) • The TSH receptor • thyroid-stimulating immunoglobulins • thyrotropin receptor-blockingimmunoglobulins
Radioiodineuptake • High uptake indicates increased new hormone synthesis by the thyroid • low uptake indicates release of preformed hormone, exogenous ingestion, or extrathyroidal hormone synthesis
Task2 • 发生甲状腺毒症可以由什么样的机制引起? • 其甲状腺相关检查的表现有什么不同? • 讨论10分钟 • 形式:分4组讨论6分钟,请另一名同学负责记录。 • 汇报形式:讨论完再由各组秘书进行抽签决定汇报顺序,每组只能讲一种机制,汇报时间不能超过1分钟,要求后面汇报的不能和前面的重复。如果是在没想出来新的机制可以选择一种机制进行补充或者纠正
Part 3 Graves disease (diffuse toxic goiter) • Most common cause of hyperthyroidism. • An autoimmune disease. • Chronic course with remissions and relapses. • Characterized by hyperthyroidism goiter exophthalmos pretibial myxedema Other autoimmune disease
Epidemiology Graves' disease can occur at any age but is unusual before puberty. It most commonly affectsthe30 to 50 year age group. The disease is more frequent in women, the ratio of predominance in women to men may be as high as 7~10: 1. Prevalence is approximately 2% of the female population.
Epidemiology Graves disease has a tendency to become manifest during puberty, pregnancy, and menopause in female. In men the disease tends to occur at a late age, to be more severe, and to be accompanied more often by ophthalmopathy and hypokalemic periodic paralysis ( especially in yellow race)
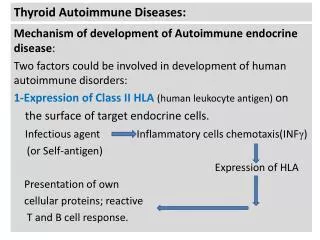
pathogenesis Genetic factors play a role. There is an association between the disease and the genes HLA ( human leucocyte antigen) B8, -DRw3, -Bw36, -Bw46, -DQA1*0501, and cytotoxic T lymphocyte associate –4(CTLA-4). Indeed, a 50% concordance is found between identical twins.
Genetic factors Infections Stress, etc Enviroment factors T3 Hypothalamus (-) T4 TRH Thyroid stimulators (TRAb) pituitary (-) TSH thyroid
pathogenesis Cytotoxic Ab Orbital Tc Orbital antigens Common orbital fibroblast- Thyroid antigen (TSH-R) B cell TSI, Tg Ab, TPO Ab Thyroid Ag Th Ts Thyroid gland David G.Gardner. Dolores Shoback. Greenspan`s basic and clinical endocrinology
甲状腺肿大可分为三度 • I度不能看出肿大但能触及 • II度能看到肿大又能触及,但在胸锁乳突肌以内 • III度超过胸锁乳突肌外缘者
Symptoms and Signs of GD Pretibial myxedema: thick redness on the front of legs (with Graves' disease) Non piting infiltration in the pretibial area. the lesion is often pruritic and erythematous in its early stages and subsequently becomes brawny.
甲状腺眼征(非浸润性突眼) • 眼球突出双侧眼球突出,也可为单侧,可不对称 • Graefe征:眼球下转时上睑不能相应下垂 • Stellwag征:瞬目减少 • Mobius征:辐辏运动减弱 • Joffroy征:上视时无额纹出现
American Thyroid Association: Assessment of GO clinical activity score (CAS) • Painfulfeelingbehindtheglobeoverlast4weeks痛 • Painwitheyemovementduringlast4wks痛 • Rednessoftheeyelids红 • Rednessofconjunctiva红 • Swellingoftheeyelids肿 • Chemosis(edemaoftheconjunctiva)肿 • Swollencaruncle肿 Increaseinproptosis≥ 2mm Decreasedeyemovements ≥ 5°anydirection Decreasedvisualacuity≥ 1lineonsnellenchart • a7-piointscale,GOisactivewithCAS≥ 3
SeverityofGO • The severity therefore ranges from 0 to VI(NOSPECS) Class 0 – No symptoms or signs Class I – Only signs, no symptoms (eg, lid retraction, stare, lid lag) Class II – Soft tissue involvement Class III – Proptosis Class IV – Extraocular muscle involvement Class V – Corneal involvement Class VI – Sight loss (optic nerve involvement)
ATDs Patients with high likelihood of remission (patients, especially females, with mild disease, small goiters, and negative or low-titer TRAb); patients with moderate to severe active GO the elderly increasing surgical risk or with limited life expectancy; patients with previously operated or irradiated necks; patients with lack of access to a high-volume thyroid surgeon HYPERTHYROIDISM MANAGEMENT GUIDELINES. ATA 2016
131I contraindications to ATD use Females planning a pregnancy in the future (in more than 4–6 months following radioiodine therapy, provided thyroid hormone levels are normal) individuals with comorbidities increasing surgical risk patients with previously operated or externally irradiated necks lack of access to a high-volume thyroid surgeon HYPERTHYROIDISM MANAGEMENT GUIDELINES. THYROID. 2011; 21, 6,
Surgery Symptomatic compression or large goiters (≥80 g); relatively low uptake of radioactive iodine; when thyroid malignancy is documented or suspected; large nonfunctioning, or hypofunctioning nodule; coexisting hyperparathyroidism requiring surgery HYPERTHYROIDISM MANAGEMENT GUIDELINES. THYROID. 2011; 21, 6,
Antithyroid drugs Methimazole(MM, tapazole , first choice): Methimazole should be used in virtually every patient who chooses antithyroid drug therapy for GD,orduringBreast feeding. Except during the first trimester of pregnancy when propylthiouracil is preferred, in the treatment of thyroid storm, and in patients with minor reactions to methimazole who refuse radioactive iodine therapy or surgery HYPERTHYROIDISM MANAGEMENT GUIDELINES. THYROID. 2011; 21, 6,
PTU( propylthiouracil) second choice,special condition
Sideeffects Patients should be informed of side effects of antithyroid drugs and the necessity of informing the physician promptly if they should develop pruritic rash, jaundice, acolic stools or dark urine, arthralgias, abdominal pain, nausea, fatigue, fever, or pharyngitis. Before starting antithyroid drugs and at each subsequent visit, the patient should be alerted to stop the medication immediately and call their physician when there are symptoms suggestive of agranulocytosis or hepatic injury or severe adverse reactions. HYPERTHYROIDISM MANAGEMENT GUIDELINES. THYROID. 2011; 21, 6,
Treatment Prior to initiating antithyroid drug therapy for GD, we suggest that patients have a baseline complete blood count, including white count with differential, and a liver profile including bilirubin and transaminases. HYPERTHYROIDISM MANAGEMENT GUIDELINES. THYROID. 2011; 21, 6,
Other Drugs Other drugs called beta-blockers (e.g. Propanolol, atenolol,metoprolol,nadolol) can be given in the early stages to control the symptoms of hyperthyroidism. When the symptoms have settled these drugs are usually stopped whilst the antithyroid drugs are continued
Treatment 2.Radioactive iodine (131I) therapy:核医学老师讲 Radioiodine treatment is often recommended once the overactive thyroid is brought under control with tablets. The great advantage of radioiodine is that it is given at an outpatient visit, as a single tasteless drink. It has little or no side effects but smoothly and painlessly cures the thyroid condition. Radioiodine is the most common form of treatment worldwide and has been in safe and effective use for 50 years.
Treatment Radioactive iodine is not given to pregnant women. Dosage of 131I is difficult to gauge. The response of the gland cannot be predicted. If sufficient 131I is given to produce euthyroidism,25% of the patients will become hypothyroidism in 1 year later, and increase yearly. If smaller doses are used, there is a higher incidence of recurrence of hyperthyroidism.
Treatment 3.Surgical treatment: (由甲状腺外科老师讲)
Graves ophthalmopathy (GO) should be treated jointly by the endocrinologist, and may require: corticosteroids immuno-suppressing agents orbital radiation or surgery. Treatment of orbitopathy