Download
1 / 34
510 likes | 673 Vues
VASCULAR ACCESS FOR HEMODIALYSIS. dr. Niko Azhari Hidayat, SpBTKV, MARS Divisi Bedah Toraks Kardiovaskular RS Universitas Airlangga Surabaya. Hemodialysis access. The number of patients with end-stage renal disease (ESRD) in the United States has increased steadily.

E N D
VASCULAR ACCESS FOR HEMODIALYSIS dr. Niko Azhari Hidayat, SpBTKV, MARS Divisi Bedah Toraks Kardiovaskular RS Universitas Airlangga Surabaya
Hemodialysis access • The number of patients with end-stage renal disease (ESRD) in the United States has increased steadily. • 2030: 2.24 million patients with ESRD. • The creation and maintenance of functioning vascular access, along with the associated complications, constitute the most common cause of morbidity, hospitalization, and cost in patients with end-stage renal disease.
Vascular System Internal Jugular Vein External Jugular Vein Superior Vena Cava Brachlocephalic Vein Subclavian Vein Cephalic Vein Axillary Vein Brachial Vein Inferior Vena Cava
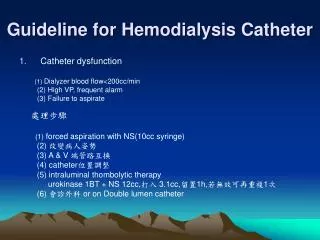
Vascular Access via Percutaneous Catheters • useful method of gaining immediate access to the circulation. • associated with higher risks. • the use-life of this type of access is shorter than that of AVFs. • Noncuffed catheters • Short term: <3 weeks
Cuffed catheters Patients who will require long-term access should have a tunneled catheter placed. allow so-called no-needle dialysis with high flow rates eliminate the problem of vascular steal placed in a subcutaneous tunnel under fluoroscopic guidance Vascular Access via Percutaneous Catheters: cuffed catheters
Vascular Access via Percutaneous Catheters: cuffed catheters • The Dacron cuff allows tissue ingrowth that helps reduce the risk of infection when compared with noncuffed catheters.
Hemodialysis access: complications • Complications can be divided into those that occur secondary to catheter placement and those that occur later. • The early complications of subclavian or internal jugular placement include pneumothorax, arterial injury, thoracic duct injury, air embolus, inability to pass the catheter, bleeding, nerve injury, and great vessel injury.
Hemodialysis access: complications • A chest radiograph must be taken after catheter placement to rule out pneumothorax and injury to the great vessels and to check for position of the catheter. • The incidence of pneumothorax is 1% to 4%,the incidence of injury to the great vessels is less than 1%. • Thrombotic complications occur in 4% to 10% of patients • Infection may occur soon after placement (3 to 5 days) or late in the life of the catheter and may be at the exit site or the cause of catheter-related sepsis. • Rate of infection between 0.5 and 3.9 episodes per 1000 catheter-days. • Catheter thrombosis increases the incidence of catheter sepsis.
Vascular Access via Arteriovenous Fistulas • Quality of life and overall outcome could be improved significantly for hemodialysis patients if two primary goals were achieved: • Increased placement of native AVFs: a minimum of 50% of new dialysis patients should have primary AVFs. • Detection of dysfunctional access before thrombosis of the access route occurs. National Kidney Foundation Dialysis Outcome and Quality Initiative (NKF-DOQI)
Vascular Access via Arteriovenous Fistulas • The ideal vascular access • permits a flow rate that is adequate for the dialysis prescription (300 ml/min), • can be used for extended periods, • and has a low complication rate. • The native AVF remains the gold standard
KDOQI- Vascular Access • 5.2 Intervention:Intervention on a fistula should be performed for the presence of: • 5.2.1 Inadequate flow to support the prescribed dialysis blood flow. (B) • 5.2.2 Hemodynamically significant venous stenosis. (B) • 5.2.3 Aneurysm formation in a primary fistula. Postaneurysmal stenosis that drives aneurysm also should be corrected. The aneurysmal segment should not be cannulated. (B) • 5.2.4 Ischemia in the access arm (B).
Arteriovenous fistulas • The standard by which all other fistulas are measured, is the Brescia-Cimino fistula. (2 year patency: 55% to 89%) • radial branch-cephalic direct access (snuffbox fistula), • autogenous ulnar-cephalic forearm transposition, • autogenous brachial-cephalic upper arm direct • access (antecubital vein to the brachial artery), • autogenous brachial-basilic upper arm transposition (basilic vein transposition). These options should be exhausted before nonautogenous material is used for dialysis access.
Noninvasive Criteria for Selection of Upper-Extremity Arteries and Veins for Dialysis Access Procedures
radiocephalic fistula (anatomic snuff-box) • radiocephalic fistula (Brescia-Cimino)
Vascular access via AVFs: • brachiocephalic fistula • brachiobasilic fistula
When is an AVF mature? • Soft firm and thin thick wall • Diameter of vessel increasing (2mm 4mm) • No collaterals detracting form the main conduit • Able to visualize and feel sites appropriate for cannulation
Prosthetic Grafts for vascular access • Upper arm grafts have a high flow rate and a low incidence of thrombosis. • higher incidence of ischemia in the hand • higher rate of stenosis, sec to endothelial hyperplasia.
Arteriovenous fistulas: Complications • Failure to mature • Stenosis at the proximal venous limb (48%). • Thrombosis (9%) • Aneurysms (7%) • Heart failure • The arterial steal syndrome and its ensuing ischemia occur in about 1.6%: pain, weakness, paresthesia, muscle atrophy, and, if left untreated, gangrene • Venous hypertension distal to the fistula : distal tissue swelling, hyperpigmentation, skin induration, and eventual skin ulceration.
Options for treating steal DRIL procedure distal revascularization-interval ligation excision of a portion of the vein plication w/ mattress or continuous sutures crossed PTFE band interposition of a 4 mm PTFE
Venous angioplasty Graft thrombolysis Treatment of venous access complications.
Contraindications to Thrombolytic Therapy • Absolute Recent major bleeding Recent stroke Recent major surgery or trauma Irreversible ischemia of end organ Intracranial pathology Recent ophthalmologic procedure • Relative History of gastrointestinal bleeding or active peptic ulcer disease Underlying coagulation abnormalities Uncontrolled hypertension Pregnancy Hemorrhagic retinopathy
HD Monitor Parameters • Dialysis Adequacy • Delivered Blood Flow • Recirculation • Vascular Access Flow • Cardiac Output
K/DOQI Guidelines for Monitoring AV Grafts and Fistulas • Access flow < 600 ml/min, the patient should be referred for fistulagram. • Access flow < 1000ml/min that has decreased by > 25% over 4 months should be referred for fistulagram.
You should do this because: Patients with AVFs live longer Patients with AVFs have 8x fewer access complications You will like: High patient and nephrologist satisfaction Simple, safe outpatient procedures Message for the Surgeon - By a SurgeonWhy only AV Fistulas? Avoid or markedly decrease hospital admissions and emergency operations for infection, bleeding, steal syndrome, and thrombosis. William Jennings, MD, Tulsa Vascular Access Surgeon
Reference: • 1.Quinton WE, Dillard D, Scribner BH: Cannulation of blood vessels for prolonged hemodialysis. Trans Am Soc Artif intern Organs 6:104, 1960 • 2. NKF-K/DOQI Clinical Practice Guidelines For Vascular Access: Guideline 29: goals of access placement – maximizing primary AV fistulae. Am J Kidney Dis 37 (Suppl 1): S169, 2001 • 3. Churchill DN, Taylor DW, Cook RI, Laplante P. Barre P. Cartier P, Fay WP, Goldstein MB, Jindal K, Mandin H, McKenzie 1K, Muirhead N, Parfrey PS, Posen GA: Canadian hemodialysis morbidity study. Am I Kidney Dis 19:214-234, 1992 • 4. Mehta S: Statistical summary of clinical results of vascular access procedures for haemodialysis, in Summer BG, Henry ML (eds): Vascular Access for Hemodialysis— II. W.L. Gore & Associates, 1991, pp 145-157 • 5. NKF-K/DOQI Clinical Practice Guidelines For Vascular Access: Guideline 3: selection of permanent vascular access and order of preference for placement of AV fistulae. Am J Kidney Dis 37 (Suppl 1): S143-144 2001 • 6. Oliver MJ, McCann RL, Indridason OS, Butterly DW, Schwab SJ. Comparison of transposed brachiobasilic fistulas to upper arm grafts and brachiocephalic fistulas. Kidney Int 60:1532-1539, 2001 • 7. Ascher E, Hingorani AP, Yorkovich WR: Techniques and outcome after brachiocephalic and brachiobasilic arteriovenous fistula creation, in A Multidisciplinary Approach for Hemodialysis Access, edited by Gray R and Sands J, New York New York, Lippincott Williams & Wilkins, 2002, pp 84-92 • 8. NKF-K/DOQI Clinical Practice Guidelines For Vascular Access: Guideline 9: access maturation. Am J Kidney Dis 37 (Suppl 1): S148-149, 2001 • 9. Pisoni RL, Young EW, Mapes DL, Keen ML, Port FK. Vascular access use and outcomes in the U.S., Europe, and Japan: results from the Dialysis Outcomes and Practice Patterns Study. Nephrol News Issues. 17:38-43, 2003
Cont’ • 10. Beathard, GA: Complications of vascular access. In: Complications of Dialysis – Recognition and Management. Edited by Lameire, N and Mehta, R. Marcel Dekker, Inc, New York. 2000, pp 1-27 • 11. Tordoir JH, Rooyens P, Dammers R, Van Der Sande FM, De Haan M, Yo TI: Prospective evaluation of failure modes in autogenous radiocephalic wrist access for haemodialysis. Nephrol Dial Transplant18:378-83, 2003 • 12. NKF-K/DOQI Clinical Practice Guidelines For Vascular Access: Guideline 8: timing of access placement. Am J Kidney Dis 37 (Suppl 1): S147-148, 2001 • 13. NKF-K/DOQI Clinical Practice Guidelines For Vascular Access: Guideline 1: Patient history and physicial examination prior to permanent access selections. Am J Kidney Dis 37 (Suppl 1): S141, 2001 • 14. Silva MB Jr, Hobson RW 2nd, Pappas PJ, Jamil Z, Araki CT, Goldberg MC, Gwertzman G, Padberg FT Jr: A strategy for increasing use of autogenous hemodialysis access procedures: impact of preoperative noninvasive evaluation. J Vasc Surg 27:302-307, 1998 • 15. Robbin ML, Gallichio MH, Deierhoi MH, Young CJ, Weber TM, Allon M. US vascular mapping before hemodialysis access placement. Radiology. 217:83-88, 2000 • 16. Allon M, Lockhart ME, Lilly RZ, Gallichio MH, Young CJ, Barker J, Deierhoi MH, Robbin ML. Effect of preoperative sonographic mapping on vascular access outcomes in hemodialysis patients. Kidney Int 60:2013-2020, 2001 • 17. Miller CD, Robbin ML, Allon M. Gender differences in outcomes of arteriovenous fistulas in hemodialysis patients. Kidney Int 63:346-352, 2003 • 18. Kamienski RW, Barnes RW: Critique of the Allen test for continuity of the palmar arch assessed by Doppler ultrasound. Surg Gynecol Obstet 142:861-864, 1976