Download
1 / 1
10 likes | 102 Vues
Integration of Tobacco Dependence into Residential Substance Abuse Treatment: Survey Results Martha Dwyer, MA, CADC, Jill Williams, MD, Jonathan Foulds, PhD, Bernice Order-Connors, LCSW, CADC, Monifa Springer, MPH. Methods The primary research questions of this evaluation were:

E N D
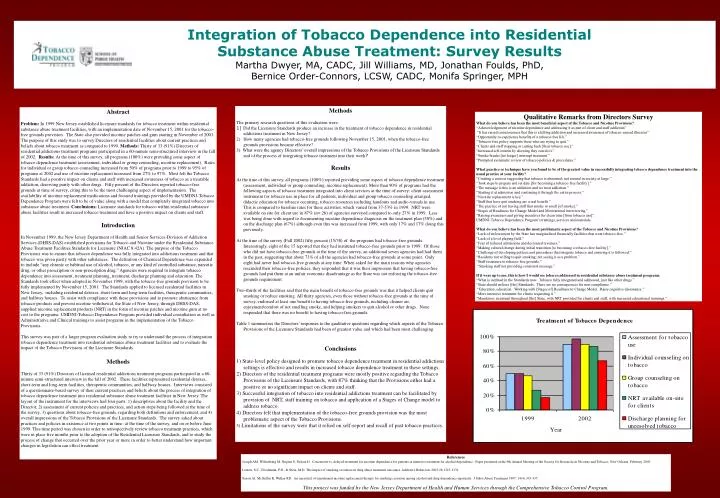
Integration of Tobacco Dependence into Residential Substance Abuse Treatment: Survey Results Martha Dwyer, MA, CADC, Jill Williams, MD, Jonathan Foulds, PhD, Bernice Order-Connors, LCSW, CADC, Monifa Springer, MPH • Methods • The primary research questions of this evaluation were: • 1) Did the Licensure Standards produce an increase in the treatment of tobacco dependence in residential • addictions treatment in New Jersey? • How many agencies had tobacco-free grounds following November 15, 2001, when the tobacco-free grounds provisions became effective? • 3) What were the agency Directors’ overall impressions of the Tobacco Provisions of the Licensure Standards and of the process of integrating tobacco treatment into their work? • Results • At the time of this survey, all programs (100%) reported providing some aspect of tobacco dependence treatment (assessment, individual or group counseling, nicotine replacement). More than 90% of programs had the following aspects of tobacco treatment integrated into client services at the time of survey: client assessment instrument for tobacco use in place for all patients, individual and group tobacco counseling arranged, didactic education for tobacco occurring, tobacco resources including handouts and audio-visuals in use. This is compared to baseline rates for these activities, which varied from 37-53% in 1999. NRT were available on site for client use in 87% (n= 26) of agencies surveyed compared to only 27% in 1999. Less was being done with regard to documenting nicotine dependence diagnosis on the treatment plan (50%) and on the discharge plan (67%) although even this was increased from 1999, with only 17% and 17% doing this previously. • At the time of the survey (Fall 2002) fifty percent (15/30) of the programs had tobacco-free grounds. Interestingly, eight of the 15 reported that they had instituted tobacco-free grounds prior to 1999. Of those who did not have tobacco-free grounds at the time of the survey, an additional seven agencies had had them in the past, suggesting that about 73% of all the agencies had tobacco-free grounds at some point. Only eight had never had tobacco-free grounds at any time. When asked for the main reasons why agencies rescinded their tobacco-free policies, they responded that it was their impression that having tobacco-free grounds had put them at an unfair economic disadvantageas the State was not enforcing the tobacco-free grounds requirement. • Two-thirds of the facilities said that the main benefit of tobacco-free grounds was that it helped clients quit smoking or reduce smoking. All thirty agencies, even those without tobacco-free grounds at the time of survey, endorsed at least one benefit to having tobacco-free grounds, including cleaner air, enjoyment/comfort of not smelling smoke, and helping smokers to quit alcohol or other drugs. None responded that there was no benefit to having tobacco-free grounds. • Table 1 summarizes the Directors’ responses to the qualitative questions regarding which aspects of the Tobacco Provisions of the Licensure Standards had been of greatest value and which had been most challenging. • Conclusions • 1) State-level policy designed to promote tobacco dependence treatment in residential addictions settings is effective and results in increased tobacco dependence treatment in these settings. • 2) Directors of the residential treatment programs were mostly positive regarding the Tobacco Provisions of the Licensure Standards, with 87% thinking that the Provisions either had a positive or no significant impact on clients and staff. • 3) Successful integration of tobacco into residential addictions treatment can be facilitated by provision of NRT, staff training on tobacco and application of a Stages of Change model to address tobacco. • 4) Directors felt that implementation of the tobacco-free grounds provision was the most problematic aspect of the Tobacco Provisions. • 5) Limitations of the survey were that it relied on self-report and recall of past tobacco practices. Abstract Problem: In 1999 New Jersey established licensure standards for tobacco treatment within residential substance abuse treatment facilities, with an implementation date of November 15, 2001 for the tobacco-free grounds provision. The State also provided nicotine patches and gum starting in November of 2001. The purpose of this study was to survey Directors of residential facilities about current practices and beliefs about tobacco treatment as compared to 1999. Methods: Thirty of 33 (91%) Directors of residential addictions treatment programs participated in a 60-minute semi-structured interview in the fall of 2002. Results: At the time of this survey, all programs (100%) were providing some aspect of tobacco dependence treatment (assessment, individual or group counseling, nicotine replacement). Rates for individual or group tobacco counseling increased from 50% of programs prior to 1999 to 95% of programs at 2002 and use of nicotine replacement increased from 27% to 97%. Most felt the Tobacco Standards had a positive impact on clients and staff with increased awareness of tobacco as a treatable addiction, deserving parity with other drugs. Fifty percent of the Directors reported tobacco-free grounds at time of survey, citing this to be the most challenging aspect of implementation. The availability of nicotine replacement medications and focused trainings provided by the UMDNJ-Tobacco Dependence Program were felt to be of value along with a model that completely integrated tobacco into substance abuse treatment. Conclusions: Licensure standards for tobacco within residential substance abuse facilities result in increased tobacco treatment and have a positive impact on clients and staff. Introduction In November 1999, the New Jersey Department of Health and Senior Services-Division of Addiction Services (DHSS-DAS) established provisions for Tobacco and Nicotine under the Residential Substance Abuse Treatment Facilities Standards for Licensure (NJAC 8:42A). The purpose of the Tobacco Provisions was to ensure that tobacco dependence was fully integrated into addictions treatment and that tobacco was given parity with other substances. The definition of Chemical Dependence was expanded to include “any chronic or habitual use of alcohol, tobacco, or any kind of controlled substance, narcotic drug, or other prescription or non-prescription drug.” Agencies were required to integrate tobacco dependence into assessment, treatment planning, treatment, discharge planning and education. The Standards took effect when adopted in November 1999, with the tobacco-free grounds provision to be fully implemented by November 15, 2001. The Standards applied to licensed residential facilities in New Jersey, including residential detoxes, short-term and long-term facilities, therapeutic communities, and halfway houses. To assist with compliance with these provisions and to promote abstinence from tobacco products and prevent nicotine withdrawal, the State of New Jersey, through DHSS-DAS, supplied nicotine replacement products (NRT) in the form of nicotine patches and nicotine gum at no cost to the programs. UMDNJ-Tobacco Dependence Program provided individual consultation as well as Administrative and Clinical trainings to assist programs in the implementation of the Tobacco Provisions. This survey was part of a larger program evaluation study to try to understand the process of integration tobacco dependence treatment into residential substance abuse treatment facilities and to evaluate the impact of the Tobacco Provisions of the Licensure Standards. Methods Thirty of 33 (91%) Directors of licensed residential addictions treatment programs participated in a 60-minute semi-structured interview in the fall of 2002. These facilities represented residential detoxes, short-term and long-term facilities, therapeutic communities, and halfway houses. Interviews consisted of a questionnaire-based survey of their current practices and beliefs about the process of integration of tobacco dependence treatment into residential substance abuse treatment facilities in New Jersey. The layout of the instrument for the interviews had four parts: 1) descriptives about the facility and the Director, 2) assessment of current policies and practices, and action steps being followed at the time of the survey, 3) questions about tobacco-free grounds, regarding both definitions and enforcement, and 4) overall impressions of the Tobacco Provisions of the Licensure Standards. The survey asked about practices and policies in existence at two points in time: at the time of the survey, and on or before June 1999. This time period was chosen in order to retrospectively review tobacco treatment practices, which were in place five months prior to the adoption of the Residential Licensure Standards, and to study the process of change that occurred over the prior year or more in order to better understand how important changes in legislation can effect treatment. Qualitative Remarks from Directors Survey What do you believe has been the most beneficial aspect of the Tobacco and Nicotine Provisions? “Acknowledgement of nicotine dependence and addressing it as part of client and staff addiction” “It has raised consciousness that this is a killing addiction and increased awareness of tobacco-caused illnesses” “Opportunity to experience benefits of a tobacco-free life.” “Tobacco-free policy supports those who are trying to quit.” “Clients and staff stopping or cutting back [their tobacco use].” “Increased self-esteem by showing they can do it.” “Smoke breaks [no longer] interrupt treatment.” “Prompted systematic review of tobacco policies & procedures.” What practice or technique have you found to be of the greatest value in successfully integrating tobacco dependence treatment into the usual practice at your facility? “Creating a context suggesting that tobacco is abnormal; not normal in society at large.” “Took steps to prepare and set date [for becoming a tobacco-free facility].” “The message is this is an addiction and we treat addiction.” “Starting it at admission and continuing it through the entire process.” “Nicotine replacement is key.” “Staff that have quit smoking are a real benefit.” “The practice of not having staff that smoke or smell [of smoke].” “Stages of Readiness for Change Model and Motivational interviewing.” “Raising awareness and giving incentives for clean time [from tobacco use]”. UMDNJ-Tobacco Dependence Program’s trainings, services and materials. What do you believe has been the most problematic aspect of the Tobacco and Nicotine Provisions? “Lack of enforcement by the State has marginalized financially facilities that went tobacco-free.” “Lack of a level playing field.” “Fear of reduced admissions and decreased revenues.” “Making cultural change during initial transition[to becoming a tobacco-free facility].” “Challenge of developing policies and procedures that integrate tobacco and ensuring it is followed.” “Residents not willing to quit smoking; not seeing it as a problem.” “Staff resistance to tobacco-free grounds.” “Smoking staff not providing consistent message.” If it were up to me, this is how I would see tobacco addressed in residential substance abuse treatment programs. “What is outlined in the Standards now. Tobacco fully integrated and addressed, just like other drugs.” “State should enforce [the] Standards. There are no consequences for non-compliance.” “Education, education. Working with [Stages of]Readiness to Change Model. Raise cognitive dissonance.” “More intensive treatment for clients requesting it.” “Mandatory treatment throughout [the] State, with NRT provided for clients and staff, with increased educational trainings.” References Joseph AM, Willenbring M, Nugent S, Nelson D. Concurrent vs. delayed treatment for nicotine dependence for patients in intensive treatment for alcohol dependence. Paper presented at the 9th Annual Meeting of the Society for Research on Nicotine and Tobacco, New Orleans, February 2003. Lemon, S.C., Friedmann, P.D., & Stein, M.D. The impact of smoking cessation on drug abuse treatment outcomes. Addictive Behaviors 2003;28:1323-1331. Saxon AJ, McGuffin R, Walker RD. An open trial of transdermal nicotine replacement therapy for smoking cessation among alcohol and drug dependence inpatients. J Subst Abuse Treatment 1997; 14(4):333-337. This project was funded by the New Jersey Department of Health and Human Services through the Comprehensive Tobacco Control Program.



















