Download
1 / 51
520 likes | 786 Vues
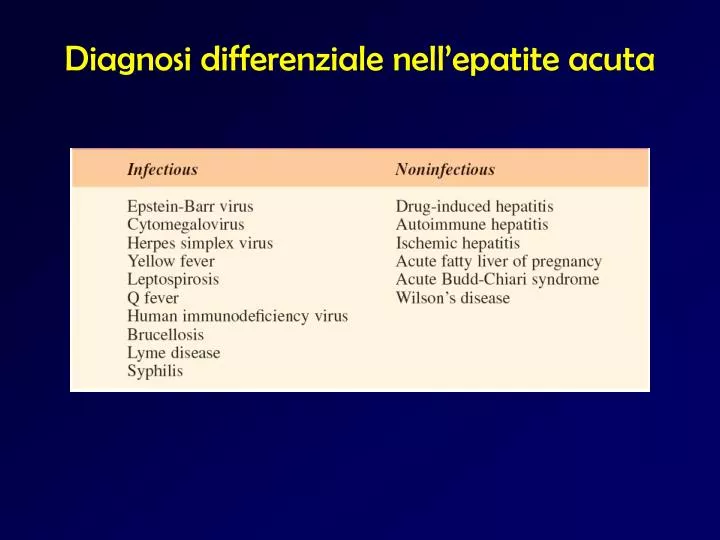
Diagnosi differenziale nell’epatite acuta. Caratteristiche dei principali virus epatitici. HAV. Il virus dell’epatite A appartiene alla famiglia delle Picornaviridae

E N D
HAV Il virus dell’epatite A appartiene alla famiglia delle Picornaviridae Inizialmente indicato come Enterovirus tipo 72, è stato quindi collocato in un genere separato, contenente una sola specie (Heparnavirus) Esiste un solo sierotipo
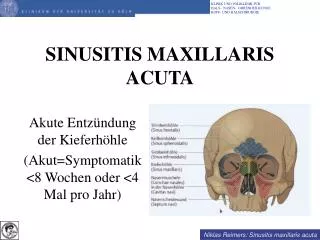
Stabilità Questo virus è stabile in un ampio range di pH ed è etere-resistente Esso viene inattivato solo parzialmente dal trattamento a 60 °C per 10-12 ore Le caratteristiche di resistenza rendono il virus adatto a persistere per un certo tempo nell’ambiente e nell’acqua
Serbatoio e trasmissione L’infezione è trasmessa per via fecale-orale
Trasmissione Il paziente è contagiante solo per un breve periodo, prima dell’esordio dei sintomi e durante la fase clinica dei prodromi La trasmissione è solitamente è mediata da acqua o cibo contaminati, talora latte (contenitori!)
Via parenterale Non ha luogo una viremia persistente, quindi la trasmissione parenterale con sangue infetto, benché possibile, risulta improbabile.
Aspetti temporali Il periodo di incubazione è 2-6 settimane L’infezione non cronicizza L’immunità post-infettiva è permanente L’infezione è comune nei i bambini, nei quali solitamente assume decorso benigno, subclinico
Soggetti e circostanze Ingestione di molluschi bivalvi provenienti da acque contaminate da acque fognarie, crudi o poco cotti Viaggi verso paesi a basso standard igienico Adulti “istituzionalizzati” Bambini che frequentano asili Omosessuali (pratiche sessuali)
Epidemie Lo scarso igiene personale e il contatto diretto hanno un ruolo fra i bambini, in particolare fra quelli che frequentano scuole ed asili. Epidemie nelle comunità sono legate all’inquinamento delle acque o alla manipolazione del cibo. Acque fognarie possono contaminare coltivazioni di ortaggi.
Vaccinazione Vaccino inattivato adsorbito Adulto: 1440 EL.U./dose (Havrix) = 1 ml o 50 U/dose = 1 ml (Vaqta); è consigliata una dose di richiamo dopo 6-12 mesi Bambino (5 mesi-10 anni): 0,5 ml; è consigliata una dose di richiamo dopo 6-12 mesi
Who Needs Vaccination for Hepatitis A? Children 2 years of age and older living in areas with high rates of hepatitis A People traveling to areas with high rates of hepatitis A Men who have sex with men Injecting and noninjecting drug users Individuals with clotting-factor disorders (eg, hemophilia) Persons with chronic liver disease People who work directly with HAV, either through handling HAV-infected primates or working directly with the virus
Global Impact of Hepatitis B 15–40% develop cirrhosis, liver failureor hepatocellular carcinoma 2 billion with past / present HBV infection 350–400 million with chronic hepatitis B World Population 6 billion Worldwide: ~1 million / year die from HBV-associated liver disease United States: Chronically infected ~1.25 million; ~5000 / year die
Global Patterns of Chronic HBV Infection • High (³8%): 45% of global population • lifetime risk of infection >60% • early childhood infections common • Intermediate(2%-7%): 43% of global population • lifetime risk of infection 20%-60% • infections occur in all age groups • Low(<2%): 12% of global population • lifetime risk of infection <20% • most infections occur in adult risk groups
The Epidemiological Triad Environment Poverty Wars Migrations Vaccination programs Virus mutants Coinfections Host Agent Aging of population Immune status
Infetti cronici • Rappresentano il principale serbatoio • Nel sangue del portatore la carica virale può essere elevatissima • Il numero degli infetti cronici assomma a 350 milioni • Questi individui continuano a produrre virus per molti anni • Fra gli infetti cronici non curati in maniera adeguata, il 25-40% è destinato a soccombere a cirrosi epatica o a carcinoma epatocellulare
Reported Geographic Distribution of Chronic HBV Infection in the ’90s Endemicity areas Carrier rate Prevalence of HBV markers High 8-20% 70-95% Intermediate 2-7% 20-55% Data as of 06.04.98 Low <2% 4-6%
Reported Geographic Distribution of Chronic HBV Infection in the New Millenium Endemicity areas Carrier rate Prevalence of HBV markers High 8-20% 70-95% Intermediate 2-7% 20-55% Low <2% 4-6%
£ 0.2% Very Low 0.3-2.0% Low 2 - 8.0% Intermediate >7.0% High No data Prevalence of HBsAg Positivity in Europe
Incidenza delle epatiti acute B e NANBItalia, 1985-2004 Casi/105 epatite B 20 epatite non-A, non-B 18 16 14 12 10 8 6 4 2 0 1985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 Dati SEIEVA
Changing frequencies of risks for HBV in Italy intrafamily horizontal blood transfusion IDU, sexual y e a r s 1970 1980 1990 2000
Trasmissione verticale • Il contagio madre-neonato è frequente soprattutto nelle aree ad elevata prevalenza • Si tratta soprattutto (90-95%) di trasmissione perinatale • attraversando il canale del parto • a seguito di trasfusione materno-fetale • Il rischio è più elevato se la madre è HBeAg+ • Il neonato va incontro ad una epatite lieve, con frequente cronicizzazione
Trasmissione parenterale • In passato, la trasmissione è stata associata a pratiche nosocomiali, • Contatto con o infusione di sangue ed emoderivati, trapianto, aghi, bisturi, lancette, siringhe, dispositivi riusabili per accesso venoso, dialisi renale • Lo scambio di aghi e siringhe fra tossicofili fornisce tuttora una via di diffusione importante
Trasmissione sessuale • L’infezione può essere contratta con il coito eterosessuale e mediante contatti omosessuali • Virus infettante è nella saliva e nello sperma • La vagina viene contaminata da sangue durante le mestruazioni; HBsAg è riconoscibile in diversi altri secreti, compresi quelli cervico-vaginali
Concentration of Hepatitis B Virus in Various Body Fluids Low/Not High Moderate Detectable blood semen urine serum vaginal fluid feces wound exudates saliva sweat tears breastmilk
Altre vie • Il virus resiste a lungo su superfici contaminate da sangue o fluidi corporei (>settimana) • Può essere trasmesso tramite stretto e prolungato contatto interpersonale (bambini, disabili mentali istituzionalizzati) • Probabile ruolo per contatto inapparente di secrezioni infette con cute non intatta o per oggetti a contatto con mucose (spazzolini, posate, stoviglie)
Burning questions: How many HBV carriers in Italy ? An estimate: from 600,000 to 900,000 How many of them with liver disease ? An estimate: about one third How many aware of their condition ? ??????
HBsAg Prevalence among pregnant women in Italy according to provenience Provenience HBsAg+/Total % Italian 139/9929 1.4 Outside EC 35/597 5.9 Unknown 8/355 2.3 Total 182/10881 1.7 Stroffolini et al. Vaccine 2003
Chronic hepatitis in hospitalised immigrants 7% 30% Africa 120 28% n. East-Europe Asia 100 South-America 80 35% 60 40 20 0 1-14 30-39 40-65 >65 15-29 AGE 2255 subjects in 48 Units 216 had chronic hepatitis HBV 41.7% HDV 0.9% HCV 37.5% Alcohol 10.2% Unknown 9.7% Scotto et al, Gruppo di Studio SIMIT, Ann Ig 2005; 17:11-18
Geographic distribution of HBV genotypes A D A C G G D B E F C A H Genetic Variability of Hepatitis B Virus 1 A2 B3 C4 D5 E6 F 7 G 8 H Genotype Sequence divergence > 8%
Clinical significance of HBV genotypes • Influence the occurrence of core/precore mutations • Spontaneous HBeAg seroconversion • B earlier than C • Sustained remission higher in genotype A than D or F • Activity of liver disease and risk of progression to cirrhosis • C > B • Response to Peg-IFNs • B – C > A > D
Antiviral-resistant HBV may generate a public health problem (?) Cross-resistance to other drugs Recurrence post-OLT Transmission to naive patients Imported from areas with high prevalence of HBV where lamivudine is extensively used as monotherapy Transmission from HIV/HBV coinfected individuals receiving lamivudine containing regimens
3.398.598 immigrati da paesi extra UE 876.300 da aree ad alta endemia HBsAg+ 10 - 13%: 87.630 – 113.918 2.506.800 da aree ad endemia intermedia HBsAg+ 5.6%: 140.380 Circa 250.000 portatori tra cittadini immigrati
Acute Hepatitis B Virus Infection with Recovery Typical Serologic Course Symptoms anti-HBe HBeAg Total anti-HBc Titer anti-HBs IgM anti-HBc HBsAg 0 4 8 12 16 24 28 32 52 100 36 20 Weeks after Exposure
Progression to Chronic Hepatitis B Virus Infection Typical Serologic Course Acute (6 months) Chronic (Years) HBeAg anti-HBe HBsAg Total anti-HBc Titer IgM anti-HBc Years 0 4 8 16 20 24 28 36 12 32 52 Weeks after Exposure