Download
1 / 24
250 likes | 444 Vues
Postoperative respiratory depression associated with the perioperative use of intrathecal morphine at Auckland Hospital. Nicola Broadbent Auckland City Hospital NZ. Aims. To examine the usage of intrathecal morphine at Auckland Hospital

E N D
Postoperative respiratory depressionassociated with the perioperative use of intrathecal morphine at Auckland Hospital Nicola Broadbent Auckland City Hospital NZ
Aims To examine the usage of intrathecalmorphine at Auckland Hospital Identify associated post-operative respiratory depression and/or sedation
Design Northern X Regional Ethics Committee and ADHB Research Office approval Retrospective 12 month period • Sept 2008 - Sept 2009 Patient group • Patients aged 16 years and over • Single dose of intrathecal morphine • Surgical procedures excluding obstetric and cardiac bypass procedures Controlled drug register Notes review to confirm administration Database compilation
Event data • 24 hr period post intrathecal morphine dose • Observations • Respiratory rate <8/min • SpO2<90% • GCS<9 • Worst AVPU score • Interventions • Medical review • sedation +/- respiratory rate • Naloxone administration • Code Red/Blue • HDU/ICU admission
Surgical speciality 429 patients underwent 438 procedures 9 patients had 2 procedures
Intrathecal morphine dose Dose range 50-500mcg Mean dose 158.5mcg Median dose 150 mcg 37 (8.4%) received a dose > 200mcg Intrathecal morphine dose (mcg)
Complications * 1 patient had preoperative hypoxia
Events by speciality High incidence of events requiring intervention in general surgical group • Hepatobilary patients responsible for all medical reviews and naloxone in this group
Hepatobiliary subgroup • Predominant group contributing to respiratory and sedation events • 36/37 received dose of 200mcg or greater • Range 175-300mcg • Mean 252 mcg • Median 250mcg
In summary • In this retrospective QA project • 12.1% had a respiratory or sedative complication • 3.4% triggered a medical review • 1.37% needed iv naloxone for respiratory depression +/- sedation • Features • Respiratory depression delayed 3.3-14.5 hr post dose • General surgical/hepatobiliary patients over-represented • Larger intrathecal morphine doses • Early iv morphine prior to PACU discharge • Gabapentin premedication • Conclusions • Orthopaedic patients can be nursed in ward setting with appropriate observations • Consider HDU placement for general surgical/hepatobiliary patients • Caution with early opiates and consider short acting opiates (egfentanyl) for bridging • Caution with gabapentin premedication
Optimum dosing • Optimization of the Dose of Intrathecal Morphine in Total Hip Surgery: A Dose-Finding Study • Robert Slappendel et al. Anesth Anal 1999 88:822-6 • 143 pt receiving either 25,50,100,200mcg followed for 24hr • Optimal dose as low as 0.1mg. • 0.2mg did not improve analgesia but increased side effects • Optimizing the dose of Intrathecal Morphine in Older Patients Undergoing Hip Arthroplasty • Laffey et al Anesth Anal 2003. 97: 1709-15 • 60 pt receiving either 0, 50, 100, 200mcg followed for 24hr • 100mcg morphine provides best balance between analgesic efficacy • Minimal effective dose of Intrathecal morphine for Pain Relief Following Transabdominal Hysterectomy • Watanabe et al Anesth Anal 1989 • 188 pt receiving 30,40,60,80,100mcg followed for 48hr • Effective analgesia at 40mcg.
Hepatobiliary patients in the literature • 2 recent studies • The use of intrathecal morphine for postoperative pain relief after liver resection: A comparison with epidural analgesia • De Pietri et al Anesth Anal 2006 • A change in practice from epidural to intrathecal morphine analgesia for hepato-pancreato-biliary surgery • Sakowska et al World J Surg 2009
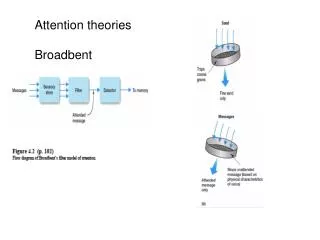
Defining respiratory depression • What do we mean? • Inadequate ventilation? • Bradypnoea? • Failure to oxygenate and clear waste gases? • What can we measure on the ward? • Definitions of "respiratory depression" with intrathecal morphine postoperative analgesia: a review of the literature • Goldstein et al. Can J Anesth 2003 • 96 studies • 46% did not define “respiratory depression” when used • 25% defined by respiratory rate alone • SpO2, ABG, naloxone treatment, carbon dioxide stimulation, level of sedation
Data collected • Patient demographics • Intrathecal morphine dose • Surgical and anaesthetic details • Other opioids • Early morphine consumption • prior to PACU discharge • Presence/absence of PCA • Opioid usage over 24hr • Sedative co-analgesics • Gabapentin premedication • Ketamine • Clonidine • Dexmedetomidine • Pain scores
Bradypnoea (APS guidelines) • Local guidelines recommend treatment with naloxone if RR <8/min and unrousable • 5.2% had a RR of <8/min documented • 1.7% on surgical ward • 1 given naloxone