Download
1 / 13
130 likes | 335 Vues
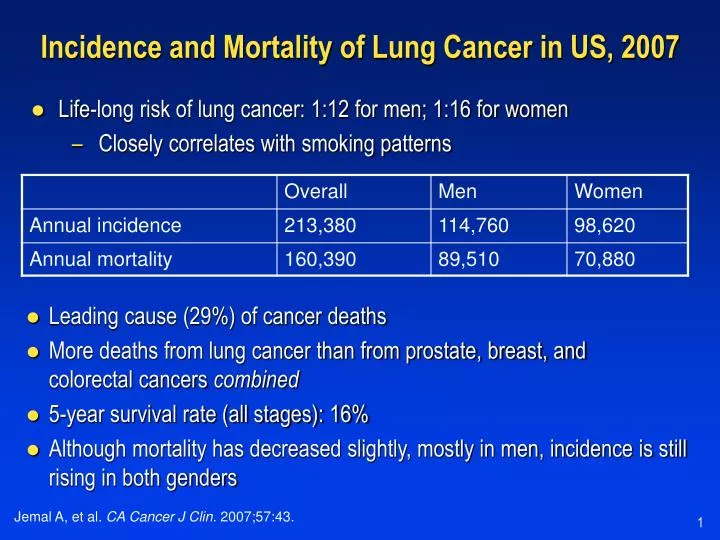
Incidence and Mortality of Lung Cancer in US, 2007. Life-long risk of lung cancer: 1:12 for men; 1:16 for women Closely correlates with smoking patterns. Leading cause (29%) of cancer deaths More deaths from lung cancer than from prostate, breast, and colorectal cancers combined

E N D
Incidence and Mortality of Lung Cancer in US, 2007 • Life-long risk of lung cancer: 1:12 for men; 1:16 for women • Closely correlates with smoking patterns • Leading cause (29%) of cancer deaths • More deaths from lung cancer than from prostate, breast, and colorectal cancers combined • 5-year survival rate (all stages): 16% • Although mortality has decreased slightly, mostly in men, incidence is still rising in both genders Jemal A, et al. CA Cancer J Clin. 2007;57:43.
TNM Staging of NSCLC T = primary tumor; N = nodal involvement; M = distant metastasis. Mountain CF. Chest. 1997;111:1710.
TNM Staging of NSCLC (cont’d) T = primary tumor; N = nodal involvement; M = distant metastasis. Mountain CF. Chest. 1997;111:1710.
Lung Cancer Histology • NSCLC • 80%–85% of all lung cancers1 • NSCLC types: squamous cell, adenocarcinoma, large cell • SCLC • 15% of all lung cancers2 • Incidence declining Small Cell3 15% Squamous Cell3 25%–30% Large Cell3 10%–15% Adenocarcinoma3 40% 1. http://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf. 2. http://www.nccn.org/professionals/physician_gls/pdf/sclc.pdf. 3. http://www.cancer.org/docroot/CRI/content/CRI_2_2_1x_What_Is_Non-small_Cell_Lung_Cancer.asp
5-Year Survival with Lung Cancer in the US Actual (%) Target (%) Limited SCLC 15–25 25–30 Extensive SCLC <1 2–5 Stage IA NSCLC 70–85 85–95 Stage IB NSCLC 60–70 70–85 Stage IIA NSCLC 35–45 45–60 Stage IIB NSCLC 25–35 35–45 Stage IIIA NSCLC 5–20 20–30 Stage IIIB NSCLC 3–7 10–20 Stage IV NSCLC <1 2–5 DeVita Jr VT, Hellman S, Rosenberg SA, eds. Cancer of the Lung. In: Cancer: Principles & Practice of Oncology. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2005;chap 31.
Limited SCLCCombination Chemotherapy and RT • EP chemotherapy combined with concurrent chest RT is well studied in limited disease • Little treatment-related mortality Coop Group Comparison Regimen(s) 5-Year Overall Survival (%) JCOG1 Concurrent vs sequential EP/RT > EPRT 24 vs 18 NCI-C2 Early vs delayed concurrent CAV/EP/RTC2 > CAV/EP/RTC6 20 vs 10 ECOG/RTOG3 BID vs QD concurrent EP/BID RT (45 Gy) > EP/QD (45 Gy) RT 26 vs 16 CAV = cyclophosphamide/doxorubicin/vincristine; EP = etoposide/cisplatin; RT = radiation therapy. 1. Takada M, et al. J Clin Oncol. 2002;20:3054. 2. Murray N, et al. J Clin Oncol. 1993;11:336. 3. Turrisi AT, et al. N Engl J Med. 1999;340:265.
Limited Stage EP (4 cycles) Concurrent chest RT PCI for CR Clinical trials Extensive Stage EP (IP) or EP/CAV (4–6 cycles) CNS metastases: chemotherapy or RT Bone metastases or obstructing lesions: RT “Window of opportunity” clinical trials SCLC Standard Therapy EP = etoposide/cisplatin; RT = radiation therapy; PCI = prophylactic cranial irradiation; CR = complete responder; IP = irinotecan/cisplatin; CAV = cyclophosphamide/doxorubicin/vincristine. Courtesy of Corey L. Langer, MD.
Current Treatment Options for NSCLC Stage I(LocalizedDisease) Surgery Adjuvant Treatmenta,b TreatmentAlgorithmfor NSCLC Stage II(LocalizedDisease) Radiation Therapy(If Unsuitable for Surgery) Adjuvant therapy for stage IB is controversial. Post hoc subgroup analyses from CALGB and NCI-C suggest that there may be a benefit to adjuvant therapy for tumors ≥4 cm Adapted from http://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf. Courtesy of Corey L. Langer, MD.
Stage-Specific Hazard Ratios for SurvivalRecent Adjuvant Trials Positive Negative Not tested Indeterminate 1. Arriagada R, et al. N Engl J Med. 2004;350:351. 2. Winton T, et al. N Engl J Med. 2005;352:2589-2597 3. Douillard JY, et al. Lancet Oncol. 2006;7:719. 4. Strauss GM, et al. 42nd ASCO. June 2–6, 2006. Abstract 7007. 5. Strauss GM, et al. 40th ASCO, June 5–8, 2004. Abstract 7019. 6. Kato H, et al. Proc Am Soc Clin Oncol. 2003;22. Abstract 2498. 7. Pignon JP, et al. J Clin Oncol. 2006;24(suppl). Abstract 7008.
Current Treatment Options for NSCLC (cont’d) Neoadjuvant Chemotherapy or Chemoradiation Surgery (If Suitable) Stage III(LocallyAdvanced) Consolidative Chemotherapy TreatmentAlgorithmfor NSCLC Chemotherapy + Radiation Therapy Palliative Stage IV(Metastatic) Chemotherapy +/- Targeted Therapy 1st-LineGemcitabine + Platinum-basedDocetaxel + Platinum-based Paclitaxel + Platinum-basedaVinorelbine Vinorelbine + Platinum-based 2nd-Line DocetaxelbPemetrexedc Erlotinib 3rd-Line Gefitinibd Erlotinibe aPaclitaxel/carboplatin + bevacizumab in selected patients. bAfter failure of prior platinum-based chemotherapy. CAfter prior chemotherapy. dIndicated only for those who have already demonstrated a therapeutic benefit on gefitinib. eAfter failure of both platinum-based and docetaxel chemotherapies. Adapted from http://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf
Positive Trials of Chemoradiation for Locally Advanced NSCLC • Induction: 4 (CALGB 84331; RTOG 88-08,2 French,3 UK4) • Concurrent: 3 (EORTC5; Jeremic6,7) • Concurrent vs sequential: 3 (Furuse8; RTOG9; Czech10) • Consolidation: 0 (SWOG 950411; HOG12; BTOG13) • Targeted treatment: 0 (SWOG 002314; RTOG 023415) 1. Dillman RO, et al. J Natl Cancer Inst. 1996;88:1175. 2. Sause WT, et al. J Natl Cancer Inst. 1995;87:195. 3. Le Chevalier T, et al. J Natl Cancer Inst. 1991;83:417. 4. Cullen MH, et al. J Clin Oncol. 1999;17:3188. 5. Schaake-Koning C, et al. Lung Cancer. 1994;10(suppl 1):S263. 6. Jeremic B, et al. J Clin Oncol. 1996;14:1065. 7. Jeremic B, et al. J Clin Oncol. 1995;13:452. 8. Furose K, et al. J Clin Oncol. 1999;17:2692. 9. Glisson B, et al. J Clin Oncol. 2000;18:2990. 10. Zatloukal P, et al. Lung Cancer. 2004;46:87. 11. Gandara DR, et al. J Clin Oncol. 2003;21:2004. 12. Hanna NH, et al. Abstract 7063. J Clin Oncol. 2006;24(June 20 suppl):18S. 13. Unpublished data. 14. Kelly K, et al. 41st ASCO. May 13–17. Abstract 7058. J Clin Oncol. 2005;23(June suppl):16S. 15. [please supply].
Metastatic NSCLC Survival Advances 100 90 Best Supportive Care (BSC) 80 Cisplatin 70 New Therapies 60 Percentage 50 40 30 20 10 0 0 1 3 4 5 2 Survival (yr) Courtesy of Corey L. Langer, MD.
Randomized Trials with CT +/- Targeted Therapies in Treatment-Naive NSCLC THERAPY TARGET CT GROUP COMMENT Gefitinib1 EGFR GC AstraZeneca Closed, no benefit Gefitinib2 EGFR PC AstraZeneca Closed, no benefit Erlotinib3 EGFR PC Genentech/OSI Closed, no benefit Erlotinib4 EGFR GC Genentech/OSI Closed, no benefit AG33405 MMP PC Agouron Closed, no benefit AG33406 MMP GC Agouron Closed, no benefit BMS2752917 MMP PC BMSO Closed, no benefit Lonafarnib8 FT (ras) PC Schering Closed, no benefit Isis 35219 PKC PC Isis Closed, no benefit Bexarotene10 RXR PC Ligand Closed, no benefit Bevacizumab11 VEGF PC ECOG Closed, positive EGFR = epidermal growth factor receptor; GC = gemcitabine + carboplatin; FT (ras) = farnesyl transferase (Ras protein); PKC = protein kinase C-alpha; RXR = retinoid X receptor; CT = chemotherapy; GC = gemcitabine + carboplatin; PC = paclitaxel + carboplatin. 1. Giaconne G, et al. J Clin Oncol. 2004;22:777. 2. Herbst RS, et al. J Clin Oncol. 2004;22:785. 3. Herbst RS, et al. J Clin Oncol. 2005;23:5892. 4. Gatzemeier U, et al. Abstract 7010. J Clin Oncol. 2004;22(July suppl): 7010. 5. Smylie M, et al. Abstract 1226. Proc Am Soc Clin Oncol. 2001;20:307a.6. Bissett D, et al. J Clin Oncol. 2005;23:842. 7. Leighl NB, et al. J Clin Oncol. 2005;23:2831. 8. Schering-Plough press release. Available at: http://www.prnewswire.com/cgi-bin/stories.pl?ACCT=104&STORY=/www/story/02-05-2004/0002104279&EDATE=. Accessed April 17, 2007. 9. Lynch T, et al. J Clin Oncol. 10. Blumenschein GR, et al. Abstract 7001. J Clin Oncol. 2005;23(June 1 suppl):16S. 11. Sandler A, et al. N Engl J Med. 2006;355:2542.