Download
1 / 76
800 likes | 1.35k Vues
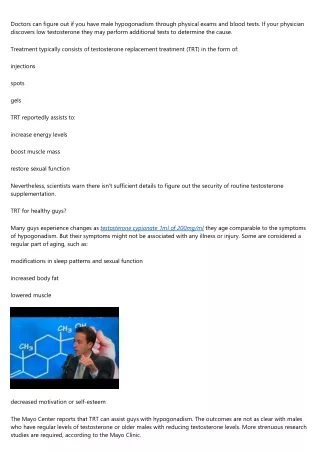
Adult Male Hypogonadism. Amy Neumeister, MD FACP. Objectives: Adult Male Hypogonadism. Screening Diagnosis/Differential Treatment Adverse events & safety monitoring. Normal Male Reproductive Axis. GnRH. Hypothalamus. FSH LH. Pituitary. Aromatase 5 reductase. Estradiol DHT.

E N D
Adult Male Hypogonadism Amy Neumeister, MD FACP
Objectives:Adult Male Hypogonadism • Screening • Diagnosis/Differential • Treatment • Adverse events & safety monitoring
Normal Male Reproductive Axis GnRH Hypothalamus FSH LH Pituitary Aromatase 5 reductase Estradiol DHT Sperm Inhibin T E Testes Seminiferous Tubule Leydig Cell
Diagnosis of Hypogonadism • Failure of testes to produce • Physiologic levels of testosterone • Normal number of spermatozoa • Primary = testes failure • Secondary = pituitary or hypothalamic failure • Dual defects are possible (less likely)
Treatment of HypogonadismDepends on the Cause • Primary hypogonadism • Generally permanent • Replace testosterone unless contradindicated • Fertility cannot be regained • Secondary hypogonadism • Distinguish cause • Evaluate for other hormone deficiencies first • Use testosterone + gonadotropins for fertility
Definition of Androgen Deficiency (AD) • Consistently low testosterone • Associated signs/symptoms • Evidence based review of literature • Data is weak at best
Don’t Screen Every Man for Low T • Don’t look for low T in men seeking care for unrelated reasons • Does not meet any criteria for general screening • No trials of efficacy or cost-effectiveness • Mortality impact of untreated low T unknown
Who to Screen for AD • Men who ask about it based on symptoms • Case finding in men with high prevalence clinical disorders • Even in these groups, data on risk/benefits of T replacement is unavailable-limited
The ADAM Questionnaire **Adapted from Morley JE, et al. Validation of a screening questionnaire for androgen deficiency in aging males. Metabolism. 2000;49(9):1239-1242.
Symptoms/Signs of AD in Men • Incomplete sexual development, eunuchoidism • Sexual desire & activity • Spontaneous erections • Breast discomfort, gynecomastia • Body hair (axillary & pubic), shaving • Very small or shrinking testes (esp < 5 ml) • Inability to father children, low/zero sperm counts • Height, low-trauma fracture, low BMD • Muscle bulk & strength • Hot flushes, sweats
Less Specific Symptoms/Signs of AD • energy, motivation, initiative, aggressiveness, self-confidence • Feeling sad or blue, depressed mood, dysthymia • Poor concentration and memory • Sleep disturbance, increased sleepiness • Mild anemia • Normochromic, normocytic, in the female range • Increased body fat, BMI • Diminished physical or work performance
Conditions with a High Prevalence of Low T (Screening Suggested) • Sellar mass, radiation to sella, other sellar disease • On meds that affect T production or metabolism • Glucocorticoids, ketoconazole, opioids • HIV-associated weight loss • ESRD and maintainence hemodialysis • Moderate to severe COPD • Osteoporosis or low trauma fracture (esp if young) • Type 2 diabetes mellitus • Infertility
Relevant Medical History • Puberty and sexual development • Past/present major illnesses • Past/present nutritional deficiency • All prescription & nonprescription drugs • Relationship problems • Sexual problems • Major life events • Related family history • Recent changes in body (breasts) • Testicle problems
Physical Exam • Amount of body hair • Breast exam for enlargement/tenderness • Size and consistency of testicles • Size of the penis • Signs of severe & prolonged AD • Loss of body hair • Reduced muscle bulk and strength • Osteoporosis • Smaller testicles
Guidelines on Screening • Initial screen = morning total testosterone • Levels are highest in the morning • Normal T is generally 300-1000 ng/dl • Confirmation = repeat morning total T • Free or bioavailable T in some • Do not screen during acute or subacute illness • Illness, malnutrition, and certain medications may temporarily lower testosterone
History and Physical (Symptoms and Signs) Morning Total T Normal T Low T Exclude reversible illness, drugs, nutritional deficiency Do you suspect altered SHBG? Not Hypogonadism Follow up Semen analysis if fertility issue Repeat T Check LH+FSH If altered SHBG Use free or bio T Normal T, LH+FSH
What lowers SHBG Moderate obesity Nephrotic syndrome Hypothyroidism Use of Glucocorticoids Progestins Androgenic steroids What raises SHBG Aging Hepatic cirrhosis Hyperthyroidism Anticonvulsants Estrogens HIV infection Testosterone Circulates Mostly Bound to Sex Hormone Binding Globulin
Confirmed low T (Total < 300 ng/dl) OR Free or Bio T < normal (Free T <5 ng/dl) Low T Low or normal LH+FSH Low T High LH+FSH Secondary Hypogonadism Primary Hypogonadism Prolactin, iron sats Other pituitary hormones Karyotype Klinefelter Syndrome Other Testicular Insult MRI in certain cases
Case • 52 y/o male with HTN asks for Viagra after 2 years of low libido • BP 150/99 • Slight gynecomastia, nl GU exam • T low, FSH &LH low, Prolactin very high • What is the best next step?
Best next step? A) Prescribe Viagra B) Testosterone replacement C) MRI pituitary D) Neurosurgery consult
When Should You Get a Pituitary MRI? • Severe secondary hypogonadism • T <150 ng/dl • Symptoms/signs of tumor mass • HA, visual impairment, visual field defect • Persistent hyperprolactinemia • Panhypopituitarism • Cost-effectiveness is unknown • Don’t bother with a CT
Should You Get a DXA? • Recommend DXA in men with • Severe androgen deficiency • Low trauma fracture • Cost-effectiveness is unknown
Goals of Testosterone Therapy • Improve/maintain secondary sexual characteristics • Improve libido and erections • Increase energy and well-being • Improve muscle mass and strength • Improve bone mineral density
Who Should be Treated with T? • Men with low T & signs/symptoms of AD • Men with low testosterone & low libido • Men with low testosterone & erectile dysfunction • After evaluation of underlying causes of ED • And consideration of other treatment for ED
Who Else Should be Treated with T? • Men with low testosterone, HIV infection & weight loss • Short-term treatment • For weight-maintenance, lean body mass, & muscle strength • Men with low testosterone & taking high dose glucocorticoids • Short-term treatment • For lean body mass and bone mineral density
What About Older Men? • Recommend against offering T to all older men with low T • Treat men with consistently low T and clinically significant symptoms • After explicit discussion of pros and cons • Task force disagreed on T level below which T should be offered to older men with symptoms • Depends on the severity of symptoms • Some T<300 • Some T<200
Case • 75 y/o male had a lower thoracic vertebral fracture after falling on a wet floor • Non-smoker, non-drinker, 1 glass milk/day • Poor energy • Libido and erections “not what they used to be” • T low x 2, LH and FSH “normal” • Anemic, normal calcium & phos • DXA T-score at L-spine -2.6, at femur -1.9 • What is the best treatment course?
Best treatment? A) Nasal calcitonin B) Bisphosphonate C) Testosterone replacement D) Calcium and Vitamin D E) Testosterone & bisphosphonate
Contraindications to Testosterone Therapy • Breast or prostate cancer • Lump/hardness on prostate exam by DRE • PSA >3 ng/ml that has not been evaluated for prostate cancer • Severe untreated BPH (AUA/IPSS >19) • Erythrocytosis (hematocrit >50%) • Hyperviscosity • Untreated obstructive sleep apnea • Severe heart failure (class III or IV)
Testosterone for the Following Reasons May be Harmful • To improve strength/athletic performance • For physical appearance • To prevent aging
How Do You Give Testosterone? • Start at standard dose • Check levels • Therapeutic target • Serum testosterone in mid-normal range for healthy, young men • Target in older men • Considerable disagreement among experts • Total T in the lower part of the normal range for younger men • 400-500 ng/dl
Nongenital Transdermal Patch • Mimics normal diurnal rhythm • Less increase in hemoglobin than IM shots • Start at 1-2 x 5 mg nightly to the skin of the back, thigh, or upper arm • Away from pressure areas • Some men need 2 patches • Skin irritation/redness/rashes
Testosterone Gel • Starting dose 5-10 grams daily • Skin tolerates it well • Potential transfer to others by skin contact • Cover the application site • Wash hands with soap and water after application • Wash skin before skin-to-skin contact with others • T levels maintained when skin washed 4-6 hours after application
Testosterone Enanthate or Cypionate Injections (IM) • T levels are supraphysiologic, then gradually drop to hypogonadal range • Peaks and valleys • Fluctuation of mood or libido • Relatively inexpensive if self-administered • Start at 75-100 mg IM weekly • Or 150-200 mg IM every other week • Pain at injection site • Excessive erythrocytosis (esp in older pts)
Buccal, Bioadhesive T Tablet • Normalizes T and DHT • 30 mg to buccal mucosa twice daily q12h • Gum-related adverse events in 16% • Gum irritation • Examine gums and oral mucosa for irritation • Alteration in taste