Download
1 / 29
290 likes | 395 Vues
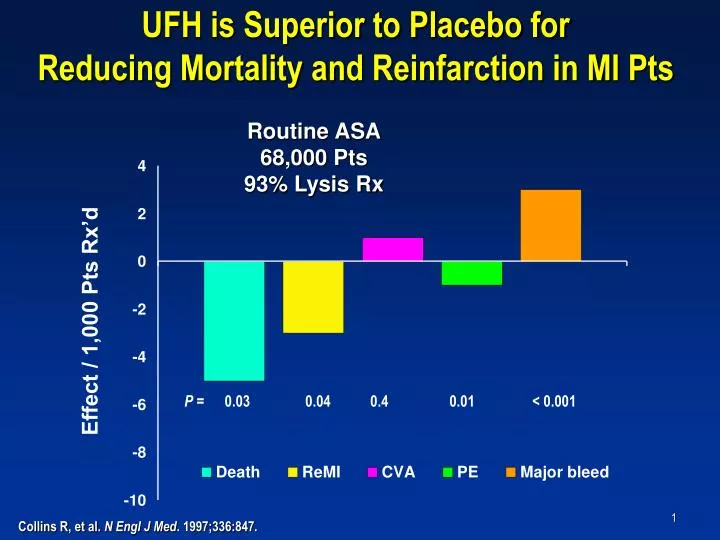
UFH is Superior to Placebo for Reducing Mortality and Reinfarction in MI Pts. Routine ASA 68,000 Pts 93% Lysis Rx. Effect / 1,000 Pts Rx’d. P = 0.03 0.04 0.4 0.01 < 0.001. Collins R, et al. N Engl J Med . 1997;336:847.

E N D
UFH is Superior to Placebo for Reducing Mortality and Reinfarction in MI Pts Routine ASA68,000 Pts93% Lysis Rx Effect / 1,000 Pts Rx’d P = 0.03 0.04 0.4 0.01 < 0.001 Collins R, et al. N Engl J Med. 1997;336:847.
LMWH is Superior to Placebo for Reducing Mortality and Reinfarction in STEMI RCTs Total Total Pts. Events LMWH Placebo 3 16,167 387 ReMI 0.76 (0.62 – 0.93) 3 16,167 1,687 Death 0.86 (0.62 – 0.93) 0.5 1 2 Favors LMWH Favors Control OR Eikelboom JW, et al. Circulation. 2005;112:3855.
Enoxaparin and Thrombolysis Reperfusion for Acute Myocardial InfarctionExTRACT-TIMI 25 ACC 2006 Atlanta, GA Disclosure Statement: Dr. Antman received research grant support via the Brigham and Women’s Hospital from sanofi-aventis This presentation reflects the views of the presenter and does not necessarily reflect the views of the American College of Cardiology. Content Distributed by Cardiosource.
Background • Advantages of ENOX over UFH Greater anti Xa:anti IIa activity Reliable A/C without monitoring Convenient sc administration • Prior trials suggestENOX may be superior to UFH • Pharmacologic reperfusion remains the most common treatment for STEMIDefinitive evaluation of ENOX vs UFH needed
Primary Hypothesis Compared to UFH, adjunctive antithrombin therapy with ENOX reduces the composite end point of all-cause mortality or non-fatal re-MI within 30 days in patients with STEMI who are eligible to receive fibrinolytic therapy.
Trial Organization TIMI Study Group Eugene BraunwaldElliott M. Antman David A. Morrow Carolyn H. McCabe Sabina Murphy Susan McHale Sponsor: sanofi-aventis Frank Jiang Christophe Gaudin Paul Chew Sylvie Fontecave Lu Cui Kim Giordano Data Safety Monitoring Board Frans Van de Werf (chair) David DeMets Desmond Julian Jean Rouleau J. Ward Kennedy Jeffrey Anderson
Protocol Design STEMI < 6 hLytic eligible Lytic choice by MD(TNK, tPA, rPA, SK) ASA Double-blind, double-dummy ENOX < 75 y: 30 mg IV bolus SC 1.0 mg / kg q 12 h (Hosp DC) ≥ 75 y: No bolusSC 0.75 mg / kg q 12 h (Hosp DC) CrCl < 30: 1.0 mg / kg q 24h UFH60 U / kg bolus (4000 U) Inf 12 U / kg / h (1000 U / h)Duration: at least 48 hCont’d at MD discretion Day 301° Efficacy Endpoint: Death or Nonfatal MI1° Safety Endpoint: TIMI Major Hemorrhage
Enrollment: Oct 2002 - Oct 2005N = 20,479 (ITT) 48 Countries 674 Sites
Baseline Characteristics-1 Characteristic ENOX(n=10,256) UFH(n=10,223) Age (yrs)-median 59 59 Male (%) 77 77 Hypertension (%) 45 44 Hyperlipidemia (%) 18 18 Current smoker (%) 47 47 Diabetes (%) 15 15 Prior MI (%) 13 13 Anterior MI (%) 44 44 ALL P = NS
Baseline Characteristics-2 Characteristic ENOX(n=10,256) UFH(n=10,223) CrCl (ml/min)-median 82 82 UFH within 3 h (%) 16 16 LMWH within 7 d (%) 0.4 0.5 Killip Class I (%) 89 89 TIMI Risk Score (STEMI) < 3 (%) 64 64 > 3 (%) 36 36 ALL P = NS
Medications Characteristic ENOX(n=10,256) UFH(n=10,223) Fibrinolytic SK (%) 20 20 Fibrin-specific (%) 80 80 TNK (%) 19 19 tPA (%) 55 55 rPA (%) 6 6 ALL P = NS
Medications Characteristic ENOX(n=10,256) UFH(n=10,223) ASA (%) 95 95 Beta Blocker (%) 86 86 ACEI / ARB (%) 80 79 Statin (%) 70 70 ALL P = NS
Primary End Point (ITT)Death or Nonfatal MI UFH 12.0% 17% RRR 9.9% ENOX Primary End Point (%) Relative Risk0.83 (0.77 to 0.90)P<0.0001 Lost to follow up = 3 Days
Treatment Benefit over Time (ITT)Death or Nonfatal MI 48 h UFH 12.0%(1223) 206 events 9.9%(1017) ENOX Primary End Point (%) 5.2% 4.7% RR0.90 (0.80 to 1.01)P=0.08 UFH ENOX Days
Major Secondary End PointDeath or Nonfatal MI or Urgent Revascularization (ITT) 48 h UFH 14.5% (1479) 280 events19% RRR 11.7% (1199) ENOX Secondary End Point (%) RR 0.81 (0.75 to 0.87)P<0.0001 6.1% 5.3% 12% RRR RR 0.88 (0.79 to 0.98)P=0.02 UFH ENOX Days
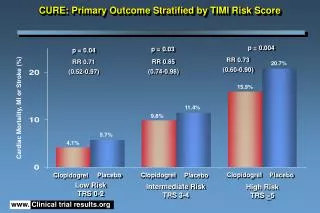
8% 33% 26% Outcomes at 30 Days (ITT) UFH ENOX % RRP value 0.920.11 0.740.0008 0.67<0.0001
2% 33% 23% Outcomes at 48 hours (ITT)Comparison of Drugs UFH ENOX % RRP value 0.980.76 0.770.086 0.670.002
Death or Nonfatal MI - Day 30 Major Subgroups Reduction In Risk (%) 18 Male SEX All Interaction TestsP = NS 16 Female 20 < 75 AGE (y) 6 >= 75 11 INFARCT Anterior LOCATION 23 Other 17 No DM B DIABETES 21 DM 17 No Prior MI B PRIOR MI 20 Prior MI 13 Streptokinase FIBRINOLYTIC 18 Fibrin-specific 23 < Median TIME TO Rx 12 > Median B 17 P < 0.0001 20,479 OVERALL 0.5 1 2 Relative Risk ENOX Better UFH Better
Death or Nonfatal MI - Day 30Medical Rx vs Any PCI 13.8 11.4 10.7RRR 23% 9.7RRR 16% % Events UFH ENOX Any PCI N = 4,676 (23%) Medical Rx N = 15,223 (75%) P Value 0.001 0.0004
Death or Nonfatal MI - Day 30Clopidogrel Use 12.2 11.4 10.4 RRR15% % Events 8.7 RRR24% UFH ENOX No Clopidogrel N = 14,752 (78%) Clopidogrel Used N = 5,727 (28%) P Value 0.0005 0.0006
Bleeding Endpoints (TIMI) 30 Days UFH ENOX ARD 0.7%RR 1.53P<0.0001 ARD 0.4%RR 1.84P = 0.001 ARD 0.4%RR 1.39P = 0.014 ARD 0.1%RR 1.27P = 0.14 % Events Major Bleed(Total) FatalMajor Bleed NonfatalMajor Bleed ICH
Net Clinical Benefit at 30 Days Prespecified Definitions UFH (%) ENOX (%) RRR (%) Death or Nonfatal MI or Nonfatal Disabl. Stroke 10.1 18 12.3 P <0.0001 Death or Nonfatal MI or Nonfatal Major Bleed 11.0 14 12.8 P <0.0001 Death or Nonfatal MI or Nonfatal ICH 10.1 17 12.2 P <0.0001 0.8 0.9 1 1.25 ENOX Better RR UFH Better
For Every 1000 Pts Treated with Enoxaparin + (No increase in nonfatal ICH) Events / 1000 Pts Nonfatal reMI Urgent Revasc. Death Nonfatal TIMI Major Bleed
Major Findings of ExTRACT-TIMI 25 • Superiority of Enoxaparin StrategySignificant reduction of ischemic events • Management of STEMIBeneficial across a wide range of subgroups Useful for medical Rx or PCI post lysis • Risks of EnoxaparinIncrease in major bleeding • Net Clinical Benefit (3 Prespecified Definitions) Significantly favors enoxaparin
Potential Explanations for Trial Results • Superior antithrombotic effect of ENOX • Longer duration of treatment with ENOX • Rebound increase in thrombotic events after discontinuingUFH
Clinical Implication A strategy ofENOX is clearly preferable to the current standard of UFH as the antithrombin to support fibrinolysis, the most common form of reperfusion for STEMI used worldwide.
Publication of Primary Results www.NEJM.org Slides and Full Listing of Trial Participants at www.TIMI.org
Trial Results In Perspective: Major Bleeding Rates Major Bleeds in Prior TrialsPooled Data UFH % Pts with Major Bleed LMWH UFH ENOX UFH ENOX UFH KeeleyLancet 2003 EikelboomCirc. 2005 Major Bleed(Total) NonfatalMajor Bleed Lytic Arms
Trial Results In Perspective:PCI vs Lysis for STEMI Overview of 23 RCTs Keeley Lancet 2003 % Events(30-42 Days) Lytic Arms (UFH) PCI Arms ENOX Reinfarction The significant advance in adjunctive therapy with enoxaparin has narrowed the gap between PCI and Lysis as reperfusion for STEMI.