Download
1 / 27
350 likes | 691 Vues
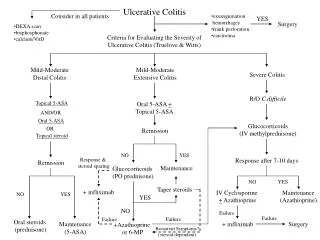
Phlebosclerotic colitis. Dr. Phillip Leung Queen Elizabeth Hospital. Case presentation. M / 69 Good past health Admitted for increased right lower quadrant pain for 3 days Associated with diarrhea Mild paraumbilical pain for 3 weeks Poor appetite for recent few months. Examination.

E N D
Phlebosclerotic colitis Dr. Phillip Leung Queen Elizabeth Hospital
Case presentation • M / 69 • Good past health • Admitted for increased right lower quadrant pain for 3 days • Associated with diarrhea • Mild paraumbilical pain for 3 weeks • Poor appetite for recent few months
Examination • BP / P stable • Afebrile • Tenderness over RLQ with rebound and guarding • PR: brownish stool, no mass • WCC 10.4, Hb 11.4 • Na 133, K 4.8, Cr 69 • Albumin 27, LFT otherwise normal • Amylase 18 • Clotting profile normal
Phlebosclerotic colitis • First reported cases by Koyama et al in 1989 in Japan; until 2000 Yao et al proposed the name “Phlebosclerotic colitis” Yao T etal (2000) Phlebosclerotic colitis: value of radiography in diagnosis–report of three cases. Radiology 214(1):188–192 • An “Asian” disease • The only “non - asian” case report is from Canada which is a gentleman who is Taiwanese by birth but a resident in Canada
Phlebosclerotic colitis • Subtype of ischemic colitis caused by venous disease; in contrast to the commoner arterial cause, namely atherosclerosis, thrombosis and embolism • Symptom is caused by chronic venous insufficiency and venous congestion secondary to phlebosclerosis • Ischemic changes lead to hemorrhage and atrophy of mucosa, submucosal fibrosis and hence motility dysfunction and stenosis of the affected colon • Right hemicolon is affected initially and gradually extends to distal colon • Superior mesenteric territories are predominantly affected with the inferior mesenteric territories largely spared, unlike the usual arterial type of ischemic colitis
Etiology • Cause of phlebosclerosis is unknown • Portal hypertension • Phlebosclerosis is an adaptive changes to increased venous pressure caused by portal hypertension • Kusanagi and Kang reported cases associated with portal hypertension Kusanagi M et al (2005) Phlebosclerotic colitis: imaging-pathologic correlation. AJR Am J Roentgenol 185(2):441–447 Kang et al (2009) Phlebosclerotic colitis in a cirrhotic patient with portal hypertension: Med Sci. 2009 Dec;24(6):1195-9. • Alcohol consumption • Ho et al. proposed alcohol consumption may play role which is his case report, cessation was associated with reduction in disease severity Ho TJ et al (2005) Phlebosclerotic colitis: an unusual cause of ischemic colitis in a 65-year-old man. J HK Coll Radiol 8:53–58 • Toxin ingestion • Causing longstanding hypoxic injury leading to necrosis of muscular coat of veins as suggested by Chang et al Chang KM et al (2007) . New histologic findings in idiopathic mesenteric phlebosclerosis. J Clin Med Assoc 2007; 70: 227–35. • Possible related condition includes • Diabetes mellitus, hyperlipidemia, cardiac disease, CREST syndrome, Churg-Strauss syndrome and lymphocytic phlebitis • Majority of patients have no associated disease and etiology remains unknown
Presentation • Relatively long period of subclinical stage which is usually irreversible and gradually deteriorative • Non – specific clinical manifestation but characteristic pathological, imaging and endoscopic findings • An under diagnosed disease • Subclinical cases were not detected mostly; real number of patients are much more than known cases
Presentation • Recurrent non specific symptom • Abdominal pain, diarrhea, constipation, nausea and vomiting, per rectal bleeding and tarry stool • Acute presentation with complication • Ileus • Mechanical obstruction • Perforation • Massive bleeding
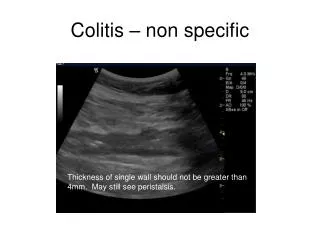
Presentation • Examination usually showed tenderness without peritoneal sign, unless complication arises • Blood test is non specific • Increased white cell count and C reactive protein • Mild increase in amylase • Abdominal XR • Multiple tortuous thread – like calcifications • Small bowel dilation and free gas
Imaging • Computed tomography • Multiple tortuous thread – like calcifications • Colonic wall thickening • Bowel dilatation or evidence of perforation Yoshikawa K et al (2009) Idiopathic phlebosclerosis: an atypical presentation of ischemic colitis treated by laparoscopic colectomy Surgery. 2009 Jun;145(6):682-4
Ba enema • Ba enema • Luminal narrowing • Thumbprinting • Disappearance of semilunar folds • Yao T etal (2000) Phlebosclerotic colitis: value of radiography in diagnosis–report of three cases. Radiology 214(1):188–192
Endoscopy • Endoscopy • Dark purple, edematous mucosa • Rigid wall • Small round ulcers • Right side colon is predominantly affected Yoshikawa K et al (2009) Idiopathic phlebosclerosis: an atypical presentation of ischemic colitis treated by laparoscopic colectomy Surgery. 2009 Jun;145(6):682-4
Hu P et al Phlebosclerotic colitis: three cases and literature review Abdom Imaging. 2013 Dec;38(6):1220-4 Jan YT et al Phlebosclerotic colitis. J Am Coll Surg. 2008 Nov;207(5):785.
CT colonoscopy Kang et al (2009) Phlebosclerotic colitis in a cirrhotic patient with portal hypertension: Med Sci. 2009 Dec;24(6):1195-9
Angiography Kang et al (2009) Phlebosclerotic colitis in a cirrhotic patient with portal hypertension: Med Sci. 2009 Dec;24(6):1195-9
Histology • Histology • Thickened and tortuous submucosal veins with fibrosis and calcified degeneration • Atrophic mucosa with hemorrhage • Fibrotic submucosa • Chronic active inflammation with wall thickening Yoshikawa K et al (2009) Idiopathic phlebosclerosis: an atypical presentation of ischemic colitis treated by laparoscopic colectomy Surgery. 2009 Jun;145(6):682-4
Treatment • No uniform standard • Conservative management was adopted for mild cases in most case report, even in progressive disease Ho TJ et al (2005) Phlebosclerotic colitis: an unusual cause of ischemic colitis in a 65-year-old man. J HK Coll Radiol 8:53–58 Hoshino Y et al (2008) Gastrointestinal: phlebosclerotic colitis. J Gastroenterol Hepatol 23(4):670. Yu CJ et al (2009) Phlebosclerotic colitis with nonsurgical treatment. Int J Colorectal Dis 24(10):1241–1242. • Hoshino followed a patient for 5 years which disease progression was noted on CT and endoscopy; patient remained asymptomatic and with no complication Hoshino Y et al (2008) Education and imaging. Gastrointestinal: Phlebosclerotic colitis J Gastroenterol Hepatol. 2008 Apr;23(4):670.
Treatment • Surgery was suggested in severe disease and complication, e.g. perforation, intestinal obstruction • Bowel resection from terminal ileum to sigmoid colon is usually required to removed all diseased bowel Kato et al (2010) Perforated phlebosclerotic colitis--description of a case and review of this condition Colorectal Dis. 2010 Feb;12(2):149-51 Markos V et al (2005) Phlebosclerotic colitis: imaging findings of a rare entity. AJR Am J Roentgenol. 2005 May;184(5):1584-6. (IO)
Take home message • Phlebosclerotic colitis is a subtype of ischemic colitis • Non – specific clinical manifestation but characteristic pathological, imaging and endoscopic findings, as simple as an abdominal XR could suggest the diagnosis • Mild disease could be managed conservatively; severe colitis with complication required surgery
Case presentation • CT report • Long segment mural thickening in ascending colon and transverse colon • Calcifications along mesenteric veins, mainly in right sided colon • Impression: phlebosclerotic colitis • 2.8cm rim enhancing collection with small extraluminal gas pocket in close association with caecum; Small 8mm defect noted in caecum • Findings suggestive of probable perforation at the caecum with associated collection
Progress • Emergency laparotomy was performed • Caecal inflammatory mass with perforation and abscess formation • Bowel gangrene from terminal ileum extending to proximal sigmoid colon • Thrombosed calcified vessels at mesentery of gangrenous bowel • Fecal peritonitis with gross contamination
Progress • Subtotal colectomy with exteriorization of small bowel and sigmoid colon performed • Post – op uneventful except wound infection • Patient’s condition gradually improved and was discharged 3 weeks after operation