Download
1 / 52
520 likes | 636 Vues
Chapters 6, 7,8. Finishing the Planning Process and Designing Interventions. Lecture by J. McKenzie. An Overview of the of Theories and Models Used. Models serve as frames from which to build; structure & organization for the planning process

E N D
Chapters 6, 7,8 Finishing the Planning Process and Designing Interventions Lecture by J. McKenzie
An Overview of the of Theories and Models Used • Models serve as frames from which to build; structure & organization for the planning process • No perfect model & no one model dominates research or practice • Approximately 10 theories and models are used regularly to plan programs • Many different theories & models; many have common elements but may have different vocabulary
Types of Theories & Models • Planning models (or theories/models of implementation) - presented in Ch. 2 • Behavior change theories (or change process theory) – “specify the relationships among casual processes operating both within and across levels of analysis (McLeroy et al., 1992, p. 3)
Behavior Change Theories • Many different change process theories • First need to decide on what level to intervene; the ecological perspective is a multilevel, interactive approach to examining the influences on health-related behaviors and conditions (Cottrell et al., 2009) • Consider the ecological perspective (McLeroy et al., 1988; Rimer & Glanz, 2005) • Intrapersonal level • Interpersonal level • Community levels: Institutional factors, Community factors, Public policy
Behavior Change Theories • Continuum theories – use an approach that identifies variables that influence action & combines them into a prediction equation (e.g., HBM, TPB) • Stage theories – are comprised of an ordered set of categories into which people can be classified, & which identifies factors that could induce movement from one category to the next (e.g., TTM, PAPM, HAPA)
Behavior Change Theories - Intrapersonal Level • This group of theories focuses on factors within the individual such as knowledge, attitudes, beliefs, self-concept, mental history, past experiences, motivation, skills, and behaviors (Glanz & Rimer, 1995) • Examples Stimulus Response, Health Belief Model, Transtheoretical Model, Precaution Adoption Process Model
Theory of Planned Behavior (TPB) • The TPB is an extension of the theory of reasoned action (TRA); it addresses the problem of incomplete volitional control • Intention – “is an indication of a person’s readiness to perform a given behavior and it is considered to be an immediate antecedent of behavior” (Ajzen, 2006) • Attitude toward the behavior – “is the degree to which performance of a behavior is positively or negatively valued” (Ajzen, 2006) • Do I really think the behavior will be good for me? • How important is the behavior to me?
Theory of Planned Behavior (TPB) • Subjective norm – “is the perceived social pressure to engage or not engage in a behavior” (Ajzen, 2006) • Do others think I should behave this way? • How much do I care what others think? • Perceived behavioral control – “refers to people’s perceptions of their ability to perform a given behavior” (Ajzen, 2006) • Do I have any control over this behavior?
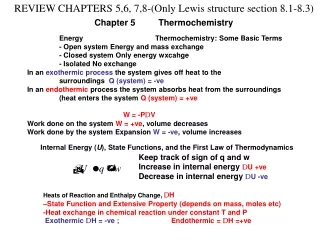
Health Belief Model (HBM) • History - developed in 1950s by Hockbaum/Kegeles/Leventhal/ Rosenstock to help explain the use of health services • Based on K. Lewin’s Decision Making model (Goal oriented/directed) • Valance - How bad you want the goal • Subjective probability - Likelihood of achieving goal based on some action • Hypothesizes: 1) health issue salient or relevant, 2) belief one is susceptible, & 3) benefits are worth the cost • The HBM “addresses a person’s perceptions of the threat of a health problem and the accompanying appraisal of a recommended behavior for preventing or managing a problem” (Rimer & Glanz, 2005, p. 12)
Health Belief Model • Constructs– • Perceived susceptibility • Perceived seriousness • Perceived barriers • Perceived benefits • Cues to action • Self-efficacy
Transtheoretical Model (TTM) • The TTM “ is an integrative framework for understanding how individuals and populations progress toward adopting and maintaining health behavior change for optimal health” (Prochaska, Johnson, & Lee, 1998, p. 59) • Has four major constructs – 1) Stages of change (this is why some call it the “Stages of Change Model”), 2) Processes of change, 3) Self-efficacy, and 4) Decisional balance
How to stage a person Do you exercise regularly? No Yes Do you intend to in the next 30 days? Have you been doing so for more than 6 months? Yes No Yes No Do you intend to in the next six months? Preparation Action Maintenance Yes No Precontemplation Contemplation
Transtheoretical Model (TTM) • Major constructs – • Stages of change • Decisional balance • Pros • Cons • Self-efficacy • Confidence • Temptation • Processes of change
Transtheoretical Model Stages of change in which processes are most emphasized
Change Process Theories - Interpersonal Level • This group of theories is comprised of theories that “assume individuals exist within, and are influenced by, a social environment. The opinions, thoughts, behavior, advice, and support of people surrounding an individual influence his or her feelings and behavior, and the individual has a reciprocal effect on those people” (Rimer & Glanz, 2005, p. 19) • Examples Social learning, social power, interpersonal communication, social networks, & social support
Social Cognitive Theory (SCT) • Builds on the SR theory • SCT describes learning as a reciprocal interaction among an individual’s environment, cognitive processes, and behavior (Parcel, 1983) • People are thinkers; expectations of consequences • Reinforcement • Direct reinforcement • Vicarious reinforcement (observational learning or social modeling) • Self-reinforcement
Often Used Constructs of the SCT • Behavior capability • Expectations • Expectancies • Locus of control • Reciprocal determinism • Self-control or self-regulation • Emotional coping response • Self-efficacy • through performance attainment (mastery of task) • through vicarious experience (observing) • as a result of verbal persuasion (suggestions from others) • through emotional arousal (interpreting one’s emotional state)
Behavior Change Theories - Community Level • This group of theories includes three of the ecological perspective levels- institutional (e.g., rules & regulations), community (e.g., social networks & norms), & public policy (e.g., legislation). • “…they explore how social systems function and change and how to mobilize community members and organizations” (Rimer & Glanz, 2005, p. 22) • Examples Theories associated with these factors include theories of community organizing and community building
Relationship of theories and models to interventions Theories Constructs Operationalize for use in interventions • Using appropriate theory & practice greatly enhances the chances of effective health promotion practice (Glanz et al., 2002)
Barriers to Applying Theory* • Failure of theory to adequately guide practice in specific settings or contexts • The lack of appropriate theories to guide community-oriented interventions • Difficulties in transferring theories from academic training context to the practice environment *Burdine & McLeory (1992)
Have a basic grasp of the theories & models Examine applicability of theories & models to the goals of the proposed program Seldom does a single theory address all the complexities of a problem Planners should select “a theory that makes sense to them, given their experience and what they know and believe about the world” (van Ryn & Heaney, 1992, p. 320) Suggestions for Applying Theory to Practice
Interventions An activity or set of activities that help to achieve the outcomes stated in the goals & objectives
Mission, Goals, & Objectives • Also called program overview or program aim • General focus • Maybe philosophy • Helps to develop goals & objectives • Don’t confuse with vision statement Mission Statement
Mission, Goals, & Objectives • General statement of intent • Future event; long-range purpose • Includes who & what Mission Statement Goals
Mission, Goals, & Objectives • Smaller steps to reach goals • More precise than goals • Written in measurable terms • Several levels Mission Statement Goals Objectives
Elements of an Objectives • Use measurable terms (Box 6.4, p. 146) • Usually verb • Avoid certain words • Some words work better with certain levels of objectives, e.g., list vs. explain Criterion (how much change) Priority Population (who) Well-written objective Conditions (when) Outcome (what) + + + =
Criteria for Developing Objectives • Realized in a reasonable time frame • Realistic? • Enough resources to reach • Consistent with policies & procedures • Don’t violate rights • Reflects the culture of priority population • In other words, are the objectives SMART? Specific, Measurable, Achievable, Realistic, Time-phased
Type Program outcome Type of Evaluation Process/Admin. Activities & tasks Process (formative) Learning Awareness, Impact (summative) knowledge, attitudes, & skills Action/Behavioral Behavior change Impact (summative) Environmental Environmental change Impact (summative) Outcome/Program Change in QOL, Outcome (summative) health status, risk, social benefits Different Levels of Objectives
Possible Criterion for an Objective* • Percent improvement • Total coverage or elimination • Consistent with another program • Projection of trend • Healthy People 2020 • Expert opinion • No increase from baseline *Gurley (2007) & USDHHS (2007b)
Intervention (treatment) • You want an intervention that is effective (leads to desired outcome) & efficient (uses resources in a responsible manner) • A theory-based strategy or experience to which those in the priority population will be exposed or in which they will take part • Has a time specific beginning and ending • Multiplicity – usually contains a number of components or activities • Dose – number of program units delivered; how many times offered
Types of Intervention Strategies • Strategy – “a general plan of action for affecting a health problem. A strategy may encompass several activities” (CDC, 2003) • CDC system of classification for strategies • More common strategies used by planners • Categories not independent of each other • Categories include: health communication, health education, health policy/enforcement, environmental change, health-related community service, community mobilization, & other
Health Communication Strategies • Health communication strategies are designed to inform & influence individual & community decisions to influence health • Usually a part of most interventions • Useful in reaching many goals & objectives • High penetration rate
Health Communication Activities Delivered in Many Ways • Computers, Internet, tailored emails • Video and audio teleconferencing • Telephones • Individual initiated - ex. help lines • Outreach - called by health educator / counselor / coach • Mass media • In person • Printed materials
Health Education Strategies • Difference between health education & health communication are not mutually exclusive categories • Health education provides the opportunity to gain in-depth knowledge about a particular health topic • Curriculum (course of study) – what those in the priority population will be taught • Scope – refers to breadth & depth of material covered • Sequence – defines the order in which the material is presented
Health Education Strategies • Units of study – “a segment of instruction focused on a particular topic” (ASCD, 2007, p. 3) • Units of study are sub-divided into lessons; outlines for the lessons are called lesson plans; lesson plans comprised of introduction, body, & conclusion • Traditional educational strategies are facilitator/learner, but there many others (e.g., self-taught, groups, technology, etc.) • Many methods for presenting lessons: lecture/discussion, group work, using audiovisuals
Health Education Strategies • Kinzie’s (2005) modification of Gagne’s “Events of Instruction” • Gain attention (convey heath threats & benefits) • Present stimulus material (tailor message to audience knowledge & values, demonstrate observable effectiveness, make behaviors easy to understand & do) • Provide guidance (use trustworthy models to demonstrate) • Elicit performance & provide feedback (for proficiency & self efficacy) • Enhance retention & transfer (social support & behavioral cues)
Health Policy / Enforcement Strategies • Includes executive orders, laws, ordinances, policies. position statements, regulations, formal / informal rules • Mandated or regulated activities; e.g., state laws to raise cigarette taxes • May be controversial; may be political, can take away freedoms, pride, $, psyche • Based on common good; protect the public’s health
Environmental Change Strategies • Those designed to change structure or types of services, or systems of care to improve delivery of health promotion (CDC, 2003) • Those things that are around the individual • Some call them health engineering strategies
Health-related Community Service Strategies • Examples include… • HRAs/HHAs • Clinical (biometric) screenings– BP, cholesterol, glucose • Services, tests, or treatments to improve health– flu shots & other immunizations • Check-ups, exams • Reduce barriers to the services – affordability, accessibility • Referrals and follow-ups are important; link with priority population’s health care providers
Community Mobilization Strategies • Community organizing – the process by which community groups are helped to identify common problems or goals, mobilize resources, and in other ways develop and implement strategies for reaching the goals they have collectively set” (Minlkler & Wallerstein, 2005, p. 26) • Community building – “an orientation to a community that is strength-based rather than need based and stresses the identification, nurturing, and celebrating of community assets” (Minkler, 2005a, p. 4) • Community advocacy – process in which those in the community become involved in the institutions & decisions that impact their lives
Community Mobilization Strategies • Advocacy activities • Voting behavior • Electioneering • Personal visits • Community rally • Lobbying • Telephone call campaigns • Use of Internet; email campaigns • TV / radio appearances to present a view • Letter-writing to key people to educate or thank • Newspaper letters to editors (congratulate / shame on you); op-ed articles
Other Strategies • Behavior Modification Activities • Systematic process • Based on SR theory • Process • Keep records (logs, diaries, journals) for a period of time • Analyze the records • Create a plan to modify the behavior
Other Strategies • Organizational Cultural Activities • Like people, organizations also have a “culture”. • Norms & traditions that are generated by & linked to the community • The culture of an organization expresses what is and what is not considered important for the organization. • Example: wellness is important
Other Strategies • Incentives (i.e., carrot; receiving) • “an anticipated positive or desirable reward designed to influence performance of an individual or group” (Chapman, 2005, p. 6) • Matching motivation & incentives • Types - social, material, miscellaneous • Disincentives (i.e., stick; taking away) • Discourages behavior • “an anticipated negative or undesirable consequence designed to influence performance of an individual or group” (Chapman, 2005, p. 6) • Can range from intrapersonal e.g., surcharge) to public policy levels (e.g., cigarette taxes)
Other Strategies • Incentives/Disincentives (continued) • Regulated by HIPAA • Employers cannot discriminate against their employees because of a “health status related factor” with the outcome affecting coverage or cost to the employee under a group or individual health plan (Chapman, 2005) • In other words, cannot deny coverage or charge employees more because of health status related conditions like high blood pressure or high blood cholesterol • But can offer incentives for participation in health promotion activities
Other Strategies • Social Support Activities • Providing support & be a willing partner • Easier to participate in a behavior with support • Types • Support groups (e.g., Weight Watchers, Overeaters Anonymous) and “buddy” systems; can be used with contests & contracts • Social activities • Social networks – a web of social relationships