Download
1 / 44
440 likes | 649 Vues
Rheumatic illnesses. As.-prof. V.Voloshyn. In Accordance with prof. Ya.Ya. Bodnar, T.V.Datsko. Rheumatic illnesses.

E N D
Rheumatic illnesses As.-prof. V.Voloshyn In Accordance with prof. Ya.Ya. Bodnar, T.V.Datsko
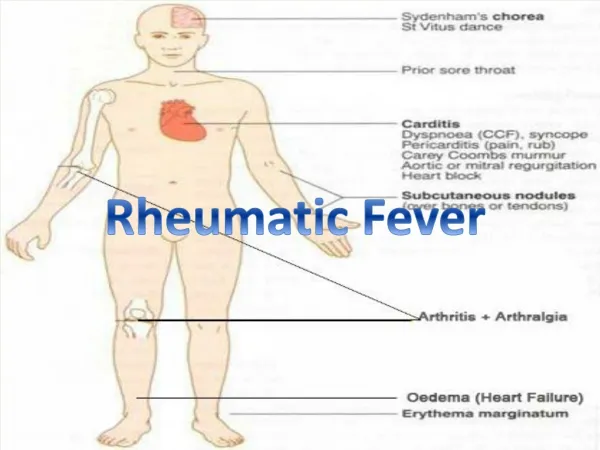
Rheumatic illnesses • -are the group of diseases in basis of development of which is the progressive system disorganization of connecting tissue and vessels, which is predefined by immune violations.
Classification of rheumatic illnesses • rheumatism; • rheumatoid arthritis (RA); • lupus erythematosus (LE); • systemic scleroderma (SS); • nodular periarteritis (NPA) and other systemic vasculites; • dermatomyositis; • illness (syndrome) of Sjogren; • illness of Bechterew (spondylitis deformans).
All rheumatic illnesses are combined by the systemic progressive damage of connecting tissue, which is characterized by stages and includes 4 types of changes:
Mucoid swelling Stages of disorganization of connecting tissue Fibrous changes Cellular reactions (granulomatic inflammation) Sclerosis
Rheumatism (Sokolsky-Bouillaud disease) is the infectiously-allergic disease which is characterized by system disorganization of connecting tissue with the dominant defeat of the heart-vessels system. An exciteris the β-haemolitic streptococcus of group A. 1-3 % of peoples which had streptococci quinsies will be ill by rheumatism. This mean that is the inclination coupled with X-chromosome.
Etiology of rheumatism The features of influencing of etiologic factor (β-haemolitic streptococcus of A group) are based in its possibility to produces the row of toxins and enzymes which can damage tissues of organism: • hyaluronidasa – increases of vascular-tissue permeability and penetration of streptococcus; • S streptolysin – damages of connecting tissue of vessels; • O streptolysin –damages connecting tissues of heart; • С-polysaccharide – has the cross antigenicity in attitude toward the connecting tissue of heart and reticuloepithelium of thymus; • M-protein – damages the cardiomyocytes up to their necrosis.
Clinico-morphologic forms of rheumatism • cardiovascular; • polyarthritic; • nodular; • cerebral.
Cardiovascular form of rheumatism • Endocarditis: valvular, chordal, atparietal; acute diffuse, acute warty, fibroplastic, relapsing warty • Myocarditis: granulomatic (nodular productive), diffuse interstitial exudative, focal interstitial exudative. • Pericarditis: serous, serofibrinous, fibrinous. • Vasculitis: capillaritis, arteriolaritis, arteritis.
The heart tends to dilate • Acute and chronic valvulitis • Mural thrombi
Morphology of Aschoff body • Is the typical lesion of rheumatic myocarditis, developing several weeks after the onset of symptoms. This structure initially consists of rounded by lymphocytes, plasma cells, macrophages, and giant cells. Eventually, the Aschoff body is replaced by a nodule of scar tissue.
Morphology of Anitschkow cells • Anitschkow cells are unusual cells within the Aschoff body, whose nuclei contain a central band of chromatin. In cross section these nuclei have an “owl eye” appearance, and when cut longitudinally trey resemble aq “caterpillar”. Anitschkow cell may become multinucleated, in which case they are termed Aschoff myocytes.
Pericarditis • Tenacious irregular deposits of fibrin are found on both the visceral and parietal surfaces of the pericardium. These deposits resemble the shaggy surfaces of two slices of buttered bread that have been pulled apart (“bread and butter pericarditis”). The pericarditis may be recognized clinically by a friction rub, but it has little functional effect and ordinarily does not lead to constrictive pericarditis.
Complications of chronic rheumatic heart disease • 1. Bacterial endocarditis follow of bacteremia, such as hose that occur during dental procedures. The scarred valves of rheumatic heart disease provide an attractive environment for bacteria that wound ordinarily bypass a normal valve • 2.Mural thrombi from in the atrial or ventricular chambers in 40% of patients with rheumatic valvular disease. They give rise to thromboemboli, which produce infarcts in various organs. Rarely, a large thrombus in the left atrial appendage develops a stalk and acts as a ball valve that obstructs the mitral valve orifice
Complications of chronic rheumatic heart disease (continuation) • 3.Congestive heart failure is associated with rheumatic disease of both the mitral and aortic valves. • 4. Cor pulmonale may develop as a result of secondary pulmonary hypertension. • 5. Adhesive pericarditis commonly follows the fibrinous pericarditis of the acute attack, but almost never results in constrictive pericarditis.
System lupus erythematosus • Lupus erythematosus (LE) is chronic polysyndrome disease mostly of young women and girls, which develops on a background the genetic predefined imperfection of immunoregulatory processes. It results to the uncontrolled productions of antibodies to own tissues and their components with development of autoimmune and immunocomplex chronic inflammation. • Morbidity by LE makes 48-50 cases per 100 thousands of population, death rate – 5,8 per 1000 000 (at this 4,7 are women).
Pathomorphology • Arteriolitis, capillaritis, vasculitis, interstitial inflammation of all internal organs with passing to the sclerosis, periarterial “bulbous” sclerosis of spleen, hyperproductions of immunoglobulins, losing of DNA, presence of lupusal cells, erythema of skin (contour of butterfly), endocarditis of Лібмана and Saxon, гломерулонефрит, поліартрит without deformation of joints
Rheumatoid arthritis • Rheumatoid Arthritis (RA) (polyarthritis)is the chronic system diseaseof connective tissue with the progressive defeat of peripheral (synovial) joints mostly as the type of erosive-destructive polyarthritis. • RА is registered in the all countries of the world and all climate-geographical areas with frequency from 0.6 to 1.3 %. Everywhere women are unwell more frequent (3-4:1).
Etiology and pathogeny • The defeat of connective tissue (mostly joints) is a result of immunopathological processes (autoaggressions). • It is consider that the violation of immune answer regulation as a result of disbalance of function of Т- and В-lymphocytes at RA is the reason of immunocomplex defeat. Because the deficit of the system of T- lymphocells leads to activating of В- lymphocells and uncontrolled synthesis of antigenes (IgG) by the plasmatic cells. Antigenes IgG at RA are changed possess [pe'zes] (володіти) autoreactivity. That is why antibodies of ІgG, ІgМ, ІgA (rheumatoid factors) act against abnormal antigenes. At interaction (co-operation) of rheumatoid factors with IgG immune complexes formed and initiate the row of chain reaction.
Pathomorphology • Arteriitis, arteriolitis, progressive destructive polyarthritis, fibrotic-bone ankilosis , osteoporosis, polyserositis (multiplemeaning), glomerulonephritis, pyelonephritis, amyloidosis of kidneys, cardiosclerosis
Systemic scleroderma (scleriasis) (Progressive systemic sclerosis) • Systemic scleroderma is the system disease of connecting tissue and small vessels, which is characterized by the widespread fibrotic-sclerotic changes of skin, stromae of internalss and symptomes of obliterated endocarditic in the form of syndrome of Reino. • Primary morbidity in the USA is known only – 12 accidents on the 1 million populations in a year. The women are unwell in 3-7 times more frequent. Age-dependent peak – 30-60 years.
Etiology and pathogeny • Etiology of Systemic scleroderma is unknown. The violation of microcirculation as a result of the defeat of vascular wall and of plasma and cellular properties of blood is the important factor of pathogeny of Systemic scleroderma. This leads to surplus synthesis of soluble forms of collogen, damage of endothelium and its substitution by smooth muscle collagen-producing , increasing of possibility to the spasm and hyperplasia of internal membrane of vessels.
Pathomorphology • Arteriitis, arteriolitis, sclerosis, hyalinosis, atrophy of skin (parchment skin), sclerodermic heart (large nidusal cardiosclerosis), sclerodermic (cortical necrosis), basal pneumofibrosis.
Nodular periarteritis • Nodular periarteritisis system necrotic vasculitis as the type segmental defeat of small and middle caliber arteries with formation of the aneurysm protrudes. The men of young age are ill mostly, morbidity makes 2-3 on the 1 million populations in the year. • Etiology. Nodular periarteritisdevelops after the acute respirators infections including the streptococcus illness,
Pathomorphology • The defeat of arteries of muscular type of small and middle calibers in the area of their fork is the most characteristic morphological sign of nodular periarteritis. The feature of nodular periarteritis is the simultaneous defeat of endothelia of vessels (deposit of immune complexes), internal elastic membrane (polymorphic-cellular inflammation contains the lymphoid epithelioid neutrophiles, fibroblasts) and perivascular tissue (cellular infiltration and scarring).